
About Authors:
N Allamneni*, CH Ajay Babu, AVS Madhulatha, C Anusha, P Sowjanya, BV Komali, M Kalyani, Syed M
*Department of Pharmaceutical Technology,
Narasaraopeta Institute of Pharmaceutical Sciences,
Narasaraopeta, Guntur, India.
*yaswanthallamneni@gmail.com
ABSTRACT
Chronopharmacokinetics involves the study of temporal changes in drug absorption, distribution, metabolism and excretion with respect to time of administration. Drug Absorption, distribution, metabolism and elimination are influenced by many different physiological functions of the body, which may vary, with time of day. Thus, the pharmacokinetic parameters characterizing these different steps, conventionally considered to be constant in time, depend on the moment of drug administration. Chronokinetic studies have been reported for many drugs in an attempt to explain chronopharmacodynamic phenomena and demonstrate that the time of administration is a possible factor of variation in the kinetics of a drug. However, the time of day has to be regarded as an additional variable influencing the kinetics of a drug since many drugs are affected by time of administration and the activity or rest period of the human or animal.
Reference Id: PHARMATUTOR-ART-1426
INTRODUCTION
The term "chrono” basically refers to the observation that every metabolic event undergoes rhythmic changes in time. Researchers have concluded that all living organisms are composites of rhythms with varying frequencies that may range from seconds to seasons. Perhaps the best-known and studied chronobiologic frequency is the circadian rhythm, which approximates the earth's 24-hour rotation around the sun. Researchers have recently concluded that both disease states and drug therapy are affected by a multitude of rhythmic changes that occur within the human body.
Chronotherapeutics refers to a treatment method in which in vivo drug availability is timed to match rhythms of disease, in order to optimise therapeutic outcomes and minimise side effects. It is based on the observation that there is an interdependent relationship between peak-to-trough rhythmic activity in disease symptoms and risk factors, pharmacologic sensitivity, and pharmacokinetics of many drugs. The specific time that patients take their medication is very important as it has significant impact on treatment success. Optimal clinical outcome cannot be achieved if drug plasma concentrations are constant. If symptoms of a disease display circadian variation, drug release should also vary over time. Drug pharmacokinetics can also be time-dependent; therefore, variations both in a disease state and in drug plasma concentration need to be taken into consideration in developing drug delivery systems intended for the treatment of disease with adequate dose at appropriate time. Various technologies such as time-controlled, pulsed, triggered and programmed drug delivery devices have been developed and extensively studied in recent years for chronopharmaceutical drug delivery.
Many functions of the human body vary considerably in a day. These variations cause changes both in disease state and in plasma drug concentrations. Human circadian rhythm is based on sleep-activity cycle, is influenced by our genetic makeup and hence, affects the body’s functions day and night (24-hour period). The dependence of bodily functions in certain disease states on circadian rhythm is well known. A number of hormones are released by the brain in the morning, while others are released during sleep. Blood pressure and heart rate are highest during the hours of 6.00 a.m. to 12.00 noon. Diseases, such as hypertension, asthma, peptic ulcer, arthritis, etc, follow the body's circadian rhythm. For example, osteoarthritis worsens during the day and is most bothersome in the evenings but for people with rheumatoid arthritis, the pain usually peaks in the morning and decreases as the day progresses.
Cardiovascular diseases such as hypertension and angina, and chest pain, also follow a definite circadian rhythm. Epidemiologic studies have documented the heightened morning-time risk of angina, myocardial infarction, and stroke. The goal in drug delivery research is to develop formulations to meet therapeutic needs relating to particular pathological conditions. Research in the chronopharmacological field has demonstrated the importance of biological rhythms in drug therapy, and this has brought a new approach to the development of drug delivery systems. Optimal clinical outcomes cannot be achieved if drug plasma concentrations are constant. If symptoms of a disease display circadian variation, drug release should also vary with time. Utilization of different technologies in the development of time controlled, pulsed, triggered and programmed drug delivery devices has intensified in recent years.
TERMINOLOGIES RELATED TO CHRONOTHERAPEUTICS
Chronotherapeutics includes the fundamentals and research into various aspects of chrono physiology, chronopathology, chronopharmacology, chrono pharmacokinetics, chronopharmacodynamics, chronoesthesy and chronotoxicology. Broadly, chronopharmaceutics bring together Chronobiology and pharmaceutics.
Chronopathology
It is the study of biological rhythms in disease processes and morbid and mortal events.
Chronopharmacology
It is the study of the manner and extent to which the kinetics and dynamics of medications are directly affected by endogenous biological rhythms, and also how the dosing time affect biological punctuality and the features (period, level, amplitude, and phase) of biological rhythms. Thus it involves both the investigation of drug effects as a function of biologic timing and the investigation of drug effects upon rhythm characteristics.
Chronopharmacokinetics
This term includes both rhythmic changes in the drug bioavailability, pharmacokinetic and its excretion.
Chronopharmacodynamics
Chronodynamics refers to dosing time, i.e., rhythm-dependent, differences in the effects of medications. Such administration- time differences are due to rhythms in the free-to-bound drug fraction, number and conformation of drug-specific receptors, ion channel dynamics, and rate limiting step(s) in metabolic pathways. Both the desired/ beneficial and undesired/adverse effects of medications can vary significantly according to their administration time.
Chronoesthesy
Chronopharmacology studies sometimes reveal great differences in their effects with different biological times of application, even through the pharmacokinetics and concentration are the same. This phenomenon is termed chronoesthesy, which is the circadian change in the susceptibility of any biosystem to a drug (including organ systems, tumors) parasites, etc.
AIM OF CHRONOPHARMACOKINETICS
The main aim of chronokinetic studies is to control the time of administration, which among others, can be responsible for variations of drug kinetics but also may explain chronopharmacological effects observed with certain drugs.
NEED FOR CHRONOPHARMACOKINETICS
There are some instances in which a chronopharmacokinetic study is needed:
* When possible daily variations in pharmacokinetics may be responsible for time dependent variations in drug effects (Ex: some antimicrobial agents are more effective at a specific time of day)
* When drugs have a narrow therapeutic range.
* When symptoms of a disease are clearly circadian phase-dependent (Ex: Nocturnal asthma, angina pectoris, myocardial infarction, ulcer disease)
* When drug plasma concentrations are well correlated to the therapeutic effect in case the latter is circadian phase-dependent
* when the drug has some serious adverse effects that can be avoided or minimized because they are related to time of administration (Ex: Aminoglycosides nephrotoxicity)
BODY RHYTHMS
These are the biological process that show cyclic variation over time. There are three types of Rhythms generally present in the human body, which was shown in Table 1.
A. Circadian Rhythms: “Circa” means about and “dies” means day.
B. Ultradian Rhythms: Oscillation of shorter duration are termed as Ultradian. (more than one cycle/day)
C. Infradian Rhythms: Oscillations that are longer than 24 h. (less than one cycle/day)
Table 1: Showing different types of Rhythms
|
S. No |
Type of Rhythm |
Example |
|
1. |
Circadian Rhythms |
Which lasts for about one day, like sleep-waking rhythm the body temperature |
|
2. |
Ultradian Rhythms |
Shorter than a day seconds (like heartbeat) |
|
3. |
Infradian Rhythms |
Longer than a day monthly rhythm-menstrual cycle yearly rhythm-bird migration |
CIRCADIAN DEPENDENCE OF DRUG KINETICS
The time of administration of a drug or toxic agent may influence the response of the organism. Chronopharmacology examines the influence of the moment of drug administration (hour, month, and year) on the drug and body response according to the temporal structure of the organism receiving it.
Thus, the quantitative response (duration or intensity of the action) of an organism, as well as the qualitative response (i.e. inhibition or induction, increase or decrease of its effect), varies with time of administration. Moreover, the different steps in pharmacokinetics, e.g. absorption, distribution, metabolism and elimination, are influenced by different physiological functions that may vary with the time of day.
Thus, pharmacokinetic parameters [including the peak drug plasma concentration [Cmax time to reach Cmax (tmax), the area under the concentration-time curve (AUC), volume of distribution (Vd), protein binding, elimination half-life (t1/2) and clearance (Cl)] which are conventionally considered to be constant in time are circadian time dependent.
More recently, Shiga et al documented differences in chronopharmacokinetic profiles between Propranolol, a lipophilic β-blocker, and Atenolol, a hydrophilic b-blocker, in patients with hypertension. Their results showed that Propranolol, but not Atenolol, is absorbed more rapidly after morning administration compared with evening administration. This confirms that the absorption rate of a lipophilic, but not a hydrophilic, drug is faster after the morning dosage in humans.
Time-dependent changes in kinetics may result from circadian variations at each step, e.g. absorption, distribution, metabolism and elimination. At each of these steps, biological rhythms may influence the kinetics of a drug, as indicated in Table 2. Circadian clock is a highly conserved feature of life on earth, imparting an approximately 24 hr period to many biological behaviours at the cellular, tissular, and organismal levels. They serve to impose internal alignments between different biochemical and physiological oscillations.
Biological functions are organized in time as rhythms with cycle durations as short as 1 second or less, as illustrated by oscillations in the electrocardiogram, and as long as 24 hours, week, month, and year. Their ability to anticipate environmental changes enables organisms to organize their physiology and behaviour such that they occur at biologically advantageous times during the day just as visual and mental acuity fluctuate, affecting complex behaviours.
The scientific study of biological rhythms and their underlying mechanisms is known as Chronobiology. The majority of health care providers are unfamiliar with this field because the teaching of biology in schools of medicine, nursing, and pharmacy is based solely on the theory of homeostasis.
Table 2: Possible Physiological factors influencing Circadian Dependent Pharmacokinetics of the Drugs
|
S. No |
Pharmacokinetics |
Physiological Factors |
|
1. |
Absorption |
Oral: Gastric pH, gastric motility, gastric emptying time, gastrointestinal blood flow, transporter. Parenteral: Transdermal permeability, ocular permeability, pulmonary permeability. |
|
2. |
Distribution |
Blood flow, albumin, α1-acid glycoprotein, red blood cells, and transporter. |
|
3. |
Metabolism |
Liver enzyme activity, hepatic blood flow, gastrointestinal enzyme. |
|
4. |
Excretion |
Renal, biliary, intestinal, Glomerular filtration, renal blood flow, urinary pH, electrolytes, tubular resorption, Transporter. |
Chronobiology, on the other hand, teaches human biological functions and processes exhibit predictable in-time cyclic variability. Emerging findings from chronobiological investigations are of such importance that re-examination of several fundamental assumptions and a practice of clinical medicine is now warranted. Many hormones in the human body are secreted in a cyclical or pulsatile manner, rather than continuously as shown in Figure 1.
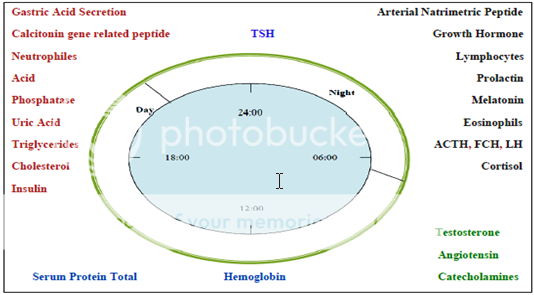
Figure 1: Human Endocrine and Exocrine secretions based on Circadian rhythm
Absorption
Absorption is altered by circadian changes in gastric empting time gastrointestinal blood flow gastric acid secretion and pH. Most lipophillic drugs seems to be absorbed faster when the drug is taken in the morning compared with the evening.
Ex: Absorption of valproic acid larger in the morning than in the evening.
Distribution
Distribution is altered by circadian changes in body size and composition blood flow to various organs drug protein binding. Peak plasma concentration of plasma proteins like albumin occurs early in the afternoon, while troughs are found during the night.
Ex: maximum binding of antineoplastics like cisplatin to plasma proteins is in afternoon and minimum in the morning.
Metabolism
Metabolism is altered by circadian changes in liver enzyme activity hepatic blood flow. Ex: For the drugs with low extraction ratio depends on liver enzyme activity and for the drugs with high extraction ratio depends on hepatic blood flow.
Excretion
Excretion is altered by circadian changes in gromerular filtration, renal blood flow, uninary pH, tubular reabsorption. All lower during the resting period than in activity period.
Ex: acidic drugs like sodium salicylate excreted quickly after evening than morning administration.
7.0 CIRCADIAN RHYTHMS IN OCCURRENCE AND SEVERITY OF DISEASES
The diseases recently targeted for pulsatile drug delivery are those, which have enough scientific background to justify chronopharmaceutical drug delivery system compared to conventional drug administration. These include asthma, arthritis, duodenal ulcer, cancer, cardiovascular diseases; diabetes, hypercholesterolemia, and neurological disorders etc., which have good circadian rhythm as shown in Figure 2.
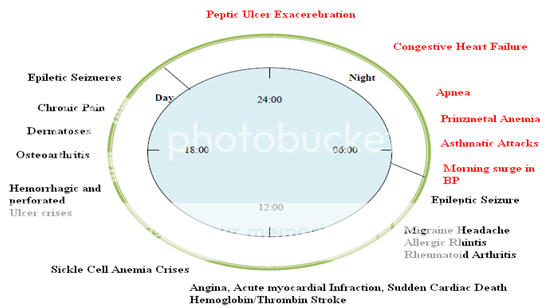
Figure 2: The Circadian Pattern of various diseases
Bronchial Asthma
It is generally identified by airway inflammation resulting in hyper responsiveness of lower respiratory tract to various environmental stimuli. It is a good target for chronotherapy because bronchoconstriction and exacerbation of symptoms vary on circadian fashion.
Allergic Rhinitis
Common symptoms of allergic rhinitis are sneezing, nasal rhinorrhea, red itchy eyes, nasal pruritus and nasal congestion. Each of the symptoms is found to occur most frequently before breakfast and in the morning and least frequently in the middle of the day. There are two phases of occurrence of allergic rhinitis i.e. early phase (developing within minutes) and late phase (manifesting after 12–16 h).
Pain
Pain control is one of the most important therapeutic priorities. Although numerous clinical practice guidelines for pain management have been published, inadequate pain relief remains a significant health care issue. It was reported that the highest threshold occurred at the end of the resting period, while the least threshold was seen at the end of the activity period. In arthritis there is circadian rhythm in the plasma concentration of C-reactive protein and Interleukin-6 of patient with rheumatoid arthritis.
Duodenal Ulcer
Generally, gastric acid secretion is highest in the evening in duodenal ulcer patients and decreases in the early mornin. Duodenal perforations showed highest incidence in the afternoon, while gastric perforations showed a major peak around noon and a secondary peak near midnight.
Cancer
There are many clock genes involved in transcriptional and post transcriptional activation and inhibition of regulatory loops that produce circadian oscillation in mammalian cells. The clock genes related rhythm alterations at the tissue level may be seen due to the desynchronization of the individual cancer cells that form into a solid tumour.
The result indicated that tumour blood flow in the night time was considerably higher than that of daytime. Although there were no marked differences in the mean arterial blood pressure, tumour size and body weight of rats between groups of daytime and night time.
Cardiovascular Diseases
In cardiovascular disease capillary resistance and vascular reactivity are higher in the morning and decreases latter in the day. Platelet agreeability is increased and Fibrinolytic activity is decreased in the morning, leading to a state of relative hypercoagulability of the blood.
Diabetes
In case of type I diabetes circadian rhythms of necessity of Insulin and its action are frequently asked question from point of physiological interest and clinical importance. Generally insulin is released in pulsatile fashion but sometimes it is irregular. Insulin can show cyclic rhythmicity of 8–30 min which can conclude optimal action. So, any difference between a daily maximum and minimum in plasma Insulin concentration besides its short-term rhythmicity has to be considered as a complex secondary circadian rhythm. It is in particular due to variable secondary early-morning and late afternoon Insulin resistance.
Hypercholesterolemia
Cholesterol synthesis is generally higher during nighttime than day light. Sometimes it varies according to individuals. The maximal production occurs early in the morning, i.e., 12 h after last meal. The activity of rate limiting enzyme HMGCoA is higher in the night time. But the diurnal variations occur due to periodicity or degradation of this regulatory enzyme.
Sleep Disorder
Many biological signaling e.g. sleep disorder occurring in the central and autonomous nervous systems show complex time structure with rhythm and pulsatile variations in multiple frequencies. The time of sleep required by each person is usually constant, although there is a wide variation among individuals. Identification of the individual variation would be of importance in dealing with certain sleep disorders.
Epilepsy
The influence of the biological clock on seizure of some partial seizures has been found in some experimental animal models. Behavioural Chronobiology provides the detection of probable new regulation processes concerning the central mechanisms of epilepsy. Because of this fact, the circadian psychophysiological patterns of epilepsy show dynamic biological systems, which recommend some intermodulating endogenous processes between observation and seizure susceptibility.
Alzheimer's Disease
Change of circadian rhythm is also seen in patients with Alzheimer's disease. Individuals with Alzheimer's show less diurnal motor activity, a higher percentage of nocturnal activity, lower inter daily stability of motor activity, and a later activity acrophase (time of peak) than normal healthy individuals. Alzheimer's disease leads to pathological changes in the suprachiasmatic nucleus and thus it disrupts circadian rhythms of the brain's function. The core body temperature is also higher in patients with this disease.
Parkinson's Disease
Autonomic dysfunction seen in Parkinson's disease discloses many alterations in circadian rhythm of blood pressure, amplified diurnal blood pressure variability and postprandial hypotension. But existence of circadian rhythm in this disease has not been evaluated. Clinical data shows daily fluctuations of motor activity pattern but the effect of the phase of the disease and the subsequent roles of drugs are difficult to estimate.
Coagulation Disorder and Thrombosis
The fluidity and retention of the blood within the circulatory system are essential for life. These dual roles are obtained through the actions and interactions of multiple variables which together form the haemostatic system. Circadian rhythm has been found in many components of circulatory and haemostatic systems such as muscle cells, aorta, peripheral vascular muscle and endothelium. The vasomotor tone of the coronary and peripheral arteries and the vasoconstrictor response to adrenaline are greater in the morning than in the afternoon.
Infectious Diseases
The elevation of body temperature, fever due to bacterial infections is higher in the evening while that due to viral infections is more likely in the morning. Influenza is epidemic in the winter season. The weight of the nasal secretions is highest in the morning in patients with cold and decreased over the day and increased again somewhat in late evening.
Table 3: Circadian rhythms and severity of Common clinical diseases
|
S. No |
Diseases |
Circadian Rhythmicity |
|
1. |
Osteoarthritis |
Symptoms worse in middle or later of the day |
|
2. |
Rheumatoid arthritis |
Most intense on awakening |
|
3. |
Peptic ulcer |
Symptoms worse in the early (sleep) am |
|
4. |
Bronchial asthma |
Exacerbations more common during sleep |
DRUGS THAT UNDERGO CHRONOPHARMACOKINETICS
Antibiotics
Many studies have reported temporal variations in the pharmacokinetics of antimicrobial drugs. Experimental animal models have shown that for Antibiotics such as beta-lactams that have concentration-independent killing effects in vitro, the time that the antibiotic concentration remains greater than the MIC(T> MIC) is themost important factor for determining the in vivo efficacy.Therefore, daily Variations in pharmacokinetics may account for impairment in the chemotherapeuticeffects.
Other important aspect of chronokinetics in antibiotics is that not only the efficacy of the drug may increase but also the toxicity of certain drugs may decrease at different time of day as we will see in aminoglycosides.The most important results in chronokinetics studies of antibiotics were given in Table 4.
Table 4: Circadian variation in the pharmacokinetics of antibiotics in human
|
S. No |
Results |
Antibiotics |
|
1. |
Higher serum levels at 9 am |
Amikacin |
|
2. |
Higher mean serum at 5 am, higher trough serum levels at 9 am |
Netilmicin |
|
3. |
Lower urine excretion at 10 pm |
Ciprofloxacin |
|
4. |
Longer serum half life at midnight |
Sulphamethoxazole |
|
5. |
Lower renal clearance at 8 pm higher renal cortex accumulation at 1:30 a.m. lower renal clearance at 1:30 am |
Amikacin |
|
6. |
Higher AUC (serum) at midnight |
Cefodizine |
Aminoglycosides
Peak renal toxicity was observed when aminoglycosides were injected in the middle of the rest period of the experimental animals, while lower toxicity was found when they were treated in the middle of the activity period. The mechanisms responsible for the temporal variation in renal toxicity of aminoglycosides are still unknown.
a. Gentamicin
Both the effectiveness and the toxicity of gentamicin varied over the 24-h Period and that the efficacy was best at the time when the toxicity of the drug was the lowest. Therefore, the administration ofgentamicin in the beginning or the middle of the day in humans may reduce renal toxicity and increase the efficacy of these antibiotics.
b. Amikacin
Amikacin in humans showed higher values for kel in the morning than in the evening.
c. Ceftriaxone
Total clearance ofceftriaxone varies rhythmicallyduring the day, with its maximumduring the dark (activity) period and its minimum during the light (rest)period in rats.
Ampicillin
Ampicillin biliary and renal clearances were significantly higher during the active cycle of rats than during the sleep cycle.
Antihypertensive Drugs
Nearly all physiological functions as well as pathophysiological events display reproducible rhythmic changes within 24 hours of a day, including the cardiovascular system. Clinical chronopharmacological studies with antihypertensive drugs gave evidence that effects on the rhythms in blood pressure and heart rate are also dependent on the time of day. Chronopharmacokinetic studies with propranolol, oxprenolol, nifedipine, verapamil, etc. also revealed daily variations in the drugs' kinetics. In general, Cmax was higher and/or tmax shorter after morning than evening dosing of these rather lipophillic drugs.
Valporic Acid
After oral administration, mean total VPA concentrations in plasma were significantly higher in the morning than in the evening during the absorption phase. Cmax tended to be higher, tmax was shorter and absorption rate constant (ka) tended to be larger for VPA in the morning than in the evening, although no difference was demonstrated in other pharmacokinetic values between morning and evening trials.
Sumatriptan
Sumatriptan is a drug of choice in migraine treatment. Migraine is a disorder that exhibits periodicity in its symptoms and so chronotherapy may be beneficial in treating the problem.
Cyclosporine
A significant delay in mean residence time was observed after the PM dose, and the PM area under the moment curve was larger than the AM value. These trends and differences suggest that more sophisticated time-dependent cyclosporine dosing methods are needed to balance AM and PM drug exposure and thereby improve immunosuppression.
Anticancer Drugs
In human bone marrow, skin, and oral and rectal mucosae, DNA synthesis, a stage of the cell-division cycle associated with increased susceptibility to S phase specific agents, decreases by 50% or more in midnight compared with daytime. The activity of dehydropyrimidine dehydrogenase in human mononuclear cells increases by 40% around midnight. This enzyme brings about the intracellular catabolism of 5-FU and contributes to improved tolerability of this drug in midnight. The chronopharmacokinetic finding of Cisplastin seems to contribute to the decreased renal toxicity during evening administration. These findings show that the circadian stage at which anticancer drugs are given to patients should be carefully considered.
NSAIDS
Studies on NSAIDs, e.g., Indomethacin and Ketoprofen, have also shown that these drugs have a greater rate and/or extent of bioavailability when they are given in the morning than when they are given in the evening due to better morning absorption. Greater blood flow of the gastrointestinal tract in the morning than in the evening may explain this phenomenon. Circadian changes in renal function, plasma protein binding or hepatic blood flow could also explain temporal variation in drug plasma levels. Many variables are known to influence pharmacokinetics.
Antiasthmatic Drugs
Antiasthmatic drugs such as Theophylline and beta sympathomimetics should be dosed higher in the evening than during daytime when asthma is predominantly nocturnal. Both the first and second-generation H1-receptor antagonists of Cyproheptadine, Terfenadine, Clemastine, and Mequitazine exerted a statistically significantly longer duration of action when they were ingested in the morning than evening.
Opioid Analgesics
Stronger analgesic effects were observed when Tramadol and Dihydrocodeine were applied in the evening to relieve painful stimuli. Finally, a recent study of Meperidine reveals a circadian variation of Meperidine-induced analgesia in sickle cell anaemia patients, with maximal analgesic effect occurring with the morning dose.
Local Anaesthetics
The duration of local anaesthesia was longest when amide-type local anaesthetic agents (Lidocaine, Ropivacaine, Mepivacaine and Betoxycaine) were applied around 3 p.m. Area under the Lidocaine plasma concentration curves (AUC) was largest in the afternoon. An administration-time-dependent variation in the transcutaneous passage of a medication was also studied. The plasma levels of Lidocaine were significantly higher in the evening than at any other time of day.
General Anaesthetics
a. Barbiturates
Higher brain pentobarbital or Hexobarbital concentrations occurred when injected during the dark phase. Postsynaptic Type-A GABAergic activity is increased during nocturnal hours, corresponding to the duration of the maximal efficacy of barbiturates.
b. Benzodiazepines
The elimination half-life of Midazolam was found to be at its shortest at 14:00 h and at its longest at 02:00.
c. Ketamine, Etomidate, Propofol, and Halogenated Agents
Action was found longer during the night than during the day. This circadian rhythm also followed a seasonal pattern between 115% in January to 54% in May– June.
d. Halothane
Greatest efficacy of Halothane occurred between 24:00 and 06:00 h.
APPLICATIONS
Treatment of Asthma
A normal lung function undergoes circadian changes and reaches a low point in the early morning hours. Chronotherapy for asthma is aimed at getting maximal effect from bronchodilator medications during early morning hours. Ex: Theophylline preparation taken once a day in the evening→blood level reaches peak.
Treatment of Gastrointestinal Disease
Gastric acid secretion is highest at night. Chronotherapy of peptic ulcers with evening once daily dosing of H2 receptor antagonist.
Ex: Ranitidine.
Treatment of Arthiritis
For osteo arthritis, ibuprofen given in the noon. The same drug will be effective when taken after the evening meal for rheumatoid arthritis.
Treatment of Cardiovascular Disease
Diseases such as hypertension, heart attack and stroke mostly occurs early in the morning. BP at its lowest during sleep cycle and rises steeply during early morning awakening period.
Treatment of Cancer
Chronobiological cycles for normal cells and tumour cells may be different.Cancer drugs administer should be timed to cycles of tumour cells making them more effective against cancer and less toxic to normal tissues. Blood flow to tumours and tumour growth rate are greater during activity phase than rest phase. By treatment at midnight more tumour cells kill could be achieved with same dose of S phase active cytotoxic therapy.
CONCLUSION
The concept of drug treatment was earlier “right drug for the right person” is now changed from Right dose for the right person to right time of dose for a right person. Drug release pattern if designed in a time-controlled manner, maximum drug can be available at peak hours with minimum side effects of toxicity.the future of kinetic studies of important and dangerous drugs as anticancer agents depend on chronokinetic since we are hopeful to find a specific time of day in which these agents are more effective and less toxic.
ACKNOWLEDGEMENT
Authors wish to give thanks to Narasaraopeta Institute of Pharmaceutical Sciences for constant support and given literature to carry out this review. Also, we would like to thank Yaswanth Allamneni of Formulation Research and Development in Natco Pharma Ltd., Hyderabad for their constant support and suggestions. We also acknowledge the help provided by our respected professors and friends in completion of the review.
REFERENCES
1. Evans R M and Marain C. Taking Your Medication: A Question of Timing. American Medical Association, 1996: 3-8
2. Evans R M, Marain C. Taking Your Medication: A Question of Timing. Chicago, IL: American Medical Association, 1996: 3-8.
3. B C Youan. Chronopharmaceutical drug delivery systems: Hurdles, hype or hope?. Adv. Drug Deliv. Rev., 2010: (62) 898-903.
4. M Rebuelto, L Ambros and M. Rubio. Daily Variationsin Ceftriaxone Pharmacokinetics in Rats. Antimicrob. Agent and chemother., 2003: (47) 809-812.
5. Michel Lebrun, Louis Grenier, Pierrette Gourde, Michel G Bergeron, Gaston Labrecque and Denis Beauchamp. Effectiveness and Toxicity of Gentamicin in an Experimental Model of Pyelonephritis: Effect of the Time of Administration. Antimicrob. Agents and chemother., 1999: (43) 1020-1026.
6. Bruguerolle B. Chronopharmacokinetics: Current status. Clin Pharmacokinet., 1998: (35) 83-94.
7. Lemmer B. Chronopharmacological aspects of PK/PD modelling. Int J Clin Pharmacol Ther., 1997: (35) 458-64.
8. Bruguerolle B and Lemmer B. Recent advances in chronopharmacokinetics: methodological problems. Life Sci., 1993: (52) 1809-1824.
9. Y Yoshiyama, S Nakano and N Ogawa. Chronopharmacokinetic study of valproic acid in man: comparison of oral and rectal administration. J clin pharmacol., 1989: 29(11) 1048-1052.
10. M H Smolensky, B Lemmer and A E Reinberg. Chronobiology and chronotherapy of allergic rhinitis and bronchial asthma. Adv. Drug Deliv. Rev., 2007: (59) 852-882.
11. R J Martin and S Banks-Schlegel. Chronobiology of asthma. Am. J. Respir. Crit. Care Med., 1998: (158) 1002-1007.
12. J G Moore and F Halberg. Circadian rhythm of gastric acid secretion in men with active duodenal ulcer. Dig. Dis. Sci., 1986: (31) 1185-1191.
13. C Svanes, R B Sothern and H Sorbye. Rhythmic patterns in incidence of peptic ulcer perforation over 5.5 decades in Norway. Chronobiol. Int., 1998: (15) 241-264.
14. F Portaluppi and B Lemmer. Chronobiology and chronotherapy of ischemic heart disease, Adv. Drug Deliv. Rev., 2007: (59) 952-965.
15. P J H Jones and D A Schoeller. Evidence for diurnal periodicity in human cholesterol synthesis. J. Lipid Res., 1990: (31) 667-673.
16. V M Kumar. Sleep and sleep disorders. Indian J. Chest Dis. Allied Sci., 2008: (50) 129-136.
17. D Beauchamp and G Labrecque. Chronobiology and chronotoxicology of antibiotics and aminoglycosides. Adv. Drug Deliv. Rev., 2007: (59) 896-903.
18. Z Khan, V Pillay, Y E Choonara and L C Du Toit. Drug delivery technologies for chronotherapeutic applications. Pharm. Dev. Technol., 2009: (14) 602-612.
19. Poondru S, Devaraj R, Boinpally R and Yamasani M R. Chronopharmacokinetics of sumatriptan in healthy human subjects. J Pharm Pharmacol,. 2000: (52) 1085-1090.
20. Aurelie Premaud, Annick Rousseau, Mireille Gicquel, Sylvie Ragot, Jacqueline Manceau, Michel Laurentie and Pierre Marquet. An Animal Model for the Study of Chronopharmacokinetics of Drugs and Application to Methotrexate and Vinorelbine. Toxicology and Applied Pharmacology, 2002: (183) 189-197.
21. Ura J, Shirachi D and Ferrill M. The chronotherapeutic approach to pharmaceutical treatment. California Pharmacist, 1992: 23(9) 46-53.
22. Halsas M, Hietala J, Veski P, Jürjenson H and Marvola M. Morning vs evening dosing of ibuprofen using conventional and time-controlled release formulations. Int J Pharm., 1999: (189) 179-185.
23. J Sajan, TA Cinu, AJ Chacko, J Litty and T Jaseeda. Chronotherapeutics and Chronotherapeutic Drug Delivery Systems. Tropical Journal of Pharmaceutical Research, 2009: 8(5) 467-475.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE








