
About Authors:
Bishal Khatiwada1,2, Binita Dhakal1,2, Surya Prasad Sharma1,2, Uddhav Timilsina1
1. Department of Biotechnology,
College for Professional Studies, Kathmandu, Nepal
2. Department of Biotechnology,
Sikkim Manipal University, Gangtok, Sikkim, India
*suryapdsharma@gmail.com
Reference Id: PHARMATUTOR-ART-1310
INTRODUCTION
Diabetes mellitus is a metabolic disorder in which person is characterized by the high blood sugar either because the body does not produce enough insulin, or because cells do not use the insulin that is produced.[1] The classical symptoms of diabetes are polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).[2] Almost one in 10 of the world population already has this condition, or can be expected to develop it during their lifetime, with prevalence rates forecast to double within the next 15 years.[3] According to WHO(2000A.D.), at least 171 million people worldwide suffer from diabetes, or 2.8% of the population.[4]
[adsense:336x280:8701650588]
There are three main types of diabetes:
Type I Diabetes: Results from the body's failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.)
Type II Diabetes: Results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency.
Gestational Diabetes: is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of T2DM.
Type II Diabetes Mellitus
Type II diabetes mellitus is also called as adult onset diabetes or non insulin dependent diabetes mellitus (NIDDM). It is less severe than type 1 or IDDM.[5] Type II diabetes mellitus is characterized by insulin resistance which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type. This Type II group comprises of approximately 90% of all cases of diabetes.[6] Most patient acquire this disease after the age of 40, but it may occur in younger people.[6] Type 2 diabetes is an emerging significant problem in children and adolescent.[7][8]
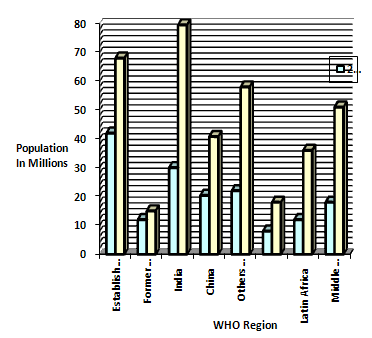
Fig1: WHO distributions of diabetic people
Type 2 diabetes is up to six times more common in people of South Asian descent and upto three times more common among people of African and African-Caribbean origin. . According to the Health Survey for England 2004, doctor-diagnosed diabetes is almost four times as prevalent in Bangladeshi men, and almost three times as prevalent in Pakistani and Indian men compared with men in the general population. [9]
Metallothionein 1A (MT1A), mRNA
Metallothionein (MT) is a sulfhydryl- and cysteine-rich protein found in microorganisms, plants and all invertebrate and vertebrate animals.
Metallothioneins are a group of ubiquitous low-molecular-weight proteins that have functional roles in cell growth, repair and differentiation. These are those family of proteins with low molecular mass and high affinity to certain metal ions.[10] They are implicated primarily in metal ion detoxification, in that they are essential for the protection of cells against the toxicity of cadmium, mercury and copper.[11]
In general the MT is known to modulate three fundamental processes:
1) The release of gaseous mediators such as hydroxyl radical or nitric oxide;
2) Apoptosis, and
3) The binding and exchange of heavy metals such as zinc, cadmium or copper.
[adsense:468x15:2204050025]
Metallothionein and Its Relationship with Diabetes
Metallothioneins (MTs) are a group of intracellular metal-binding and cysteine-enriched proteins and are highly inducible in many tissues in response to various types of stress. Although it mainly acts as a regulator of metal homeostasis such as zinc and copper in tissues, MT also acts as a potent antioxidant and adaptive (or stress) protein to protect cells and tissues from oxidative stress. Diabetes affects many Americans and other populations, and its development and toxic effect on various organs have been attributed to increased oxidative stress. Studies showed that zinc-induced or genetically enhanced pancreatic MT synthesis prevented diabetes induced by chemicals such as streptozotocin and alloxan, and zinc pretreatment also prevented spontaneously developed diabetes. Since diabetic complications are the consequences of organ damage caused by diabetic hyperglycemia and hyperlipidemia through oxidative stress, whether MT in nonpancreatic organs also provides a preventive effect on diabetic toxicity has been recently investigated. It has been demonstrated that overexpression of cardiac MT significantly prevented diabetes-induced cardiomyopathy.
Likewise, over expression of renal MT also prevented diabetes-induced renal toxicity. In addition, it was found that MT as an adaptive protein is over expressed in several organs in response to diabetes. Therefore, the biological importance of diabetes-induced MT in diabetic complications and subsequent other pathogenesis was further explored.
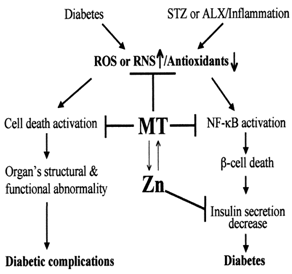
Figure2: Outline of mechanisms by which MT coordinate with Zn prevents diabetes development and diabetic complications rs8052394 of MET1A gene
This polymorphism is the result of a nucleotide change A to G at position 55231329 of chromosome 16. Similarly 225 number position of mRNA sequence, and it results in the substitution of Lysine (k) by Arginine (r) at 51 position of the MET1A protein. In the wild type, codon AAA codes for Lysine but in mutated type, codon AAA changes to AGA hence it codes for different amino acid Arginine. After analysis by MUpro we found that protein structure stability was decrease due to this polymorphism. Among the seven identified SNPs: rs8052394, rs11076161, rs8052334, rs964372, rs7191779, rs708274 and rs10636. Significant associations of MT1A rs8052394 (G alteration) with T2DM and decreased serum SOD activity were established. The other six SNPs were not significantly associated with T2DM. However, SNPs rs964372 and rs10636 were found to be significantly associated with increased serum triglyceride and neuropathy among T2DM individuals.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
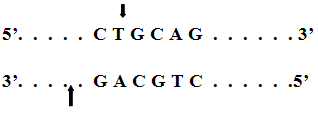
PstI
It is a restriction enzyme isolated from an E. colistrain that carries the PstI gene from Providencia stuartii 164 (ATCC 49762).
Recognition Site:
According to Nepal Diabetic Association, the number of people suffering from diabetes above 40 years in urban areas has climbed up to 19%of special note is that there will be a 67% increase in prevalence of diabetes in developing countries from 2010-2030[12].According to UN, 246 million people in the world are suffering from diabetes and approximately half of those fall in Nepal, India, China and other Asian countries. Increase in the incidence of diabetes mellitus is the 4th leading cause of death in world. Each year 3.8 million people die from diabetes and its related complication like cardiomyopathy, stroke, nephropathy, neuropathy, eye disease etc and the gene metallothionein 1A may be responsible for such complications. It has also been found that polymorphism in metallothionein 1A gene may be responsible for even inducing diabetes not only its complications[13]. Polymorphism in single nucleotide in metallothionein 1A leads for to decrease in level of SOD which may be due to the death of pancreatic β cells[14]. Metallothionein (MT) isoforms I and II are polypeptides with potent antioxidative and anti-inflammatory properties[15] and once occur polymorphism; it causes in the alteration in the normal function of the protein and causes different complications like aging, neuropathy, retinopathy, stroke etc.
Since diabetes and its complications are the 4th leading cause of death, it needs to be diagnosed soon. The most rapid results could be achieved by using molecular methods including real-time PCR, single-strand-conformation polymorphism analysis (SSCP) [16] multiplex-allele-specific PCR (MAS- PCR)[13], mass spectrophotometry, Allele-Specific Hybridization etc.But the PCR-RFLP approach has several advantages of being cheap, robust and simple to both perform and interpret, basically requiring PCR and electrophoresis set up. (Rattan A et al., 1999)
Genes significantly associated with developing type 2 diabetes, include TCF7L2, PPARG, FTO, KCNJ11, NOTCH2, WFS1, CDKAL1, IGF2BP2, SLC30A8, JAZF1, and HHEX[16][17].Within all these family, Metallothionine and its different isoforms have a relationship with T2DM and other disease like neuropathy, hyperlipidemia etc. Among different MT, the isoform MT 1A with SNP rs8052394 is found to have a significant relationship with T2DM.[16] The magnitude and trends in diabetes and the polymorphism in MT1A gene at rs8052394 are epidemiologically important to monitor, the estimation of the burden of disease is programmatically relevant in shaping policies for screening and treatment.
Methods
Study Population
63 diabetic subjects (Male: 30 Female: 32) were randomly selected within Kathmandu Valley Population. Samples collected were reported as T2DM from
Kathmandu Model Hospital, Bhrikutimandap
Samjhana Laboratory, Mangalbazzar.
Study Design
A cross sectional study was designed to explore the polymorphism in rs8052394 of MT 1A gene in T2DM patients.
Study Site
Department of Biotechnology, College for Professional Studies, Kathmandu, Nepal.
Selection of Sample
Samples reported as T2DM according to WHO criteria 2006
Criteria to Confirm T2DM
1) Age above 40 years
2) Fasting Blood Glucose: >110mg%
3) Post-prandial Glucose: >140mg%
Data Processing and Analysis
Data will be analyzed manually as well as using SPSS and interpreted according to frequency distribution and percentage. The statistical tool chi-square and t test will be applied to analyze the data. Data will be presented in tables and figures. Clinically and epidemiologically relevant information from each patient including, age, sex, dietry habits was obtained.
DNA Extraction from T2DM Samples.
D.K Lahiri et.almethod
1%Agarose Gel Electrophoresis of Extracted DNA
1% agarose gel was prepared with 0.5 µg/ml if Ethidium Bromide (EtBr) in it. 6 µl if each extracted DNA sample and the loading dye mixed in the ratio 5:1 was loaded on the wells and run for an hour at 80-90 Volt on Tris Acetate EDTA (TAE) buffer. The DNA bands were observed under UV trans-illuminator.
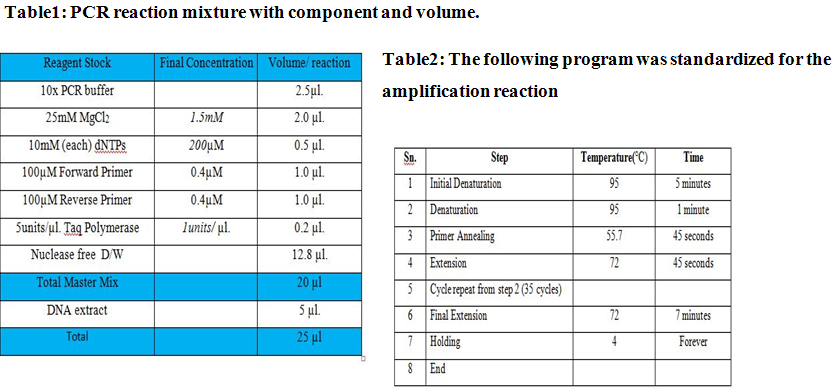
PCR Amplification of rs8052394 Specific Exon Fragment of MT1A Gene
The primary task for performing the PCR is to standardize the reaction mixture and to optimize the PCR conditions for the reaction to occur accurately so that the DNA is amplified efficiently. The reaction and the PCR programme were standardize to precisely amplify the rs8052394 specific Exon fragment of MT1A gene in the DNA sample by PCR using the primers to get a 283 bp amplified product.
Forward: 5’ACTAAGTGTCCTCTGGGGCTG 3’
Reverse: 5’AATGGGTCACGGTTGTATG3’
Procedure
2% Agarose gel electrophoresis of PCR amplified products
To check if the specific DNA segments have been amplified or not, the PCR products were electrophoresed on 2% agarose gel(0.8gm of agarose+40ml of 1X TAE buffer+0.5µg/ml of EtBr) in 1X TAE buffer along with 100bp DNA ladder(Fermentas) for 1 hour at 90 volt.
Since the specific PCR primers amplified a 283bp PCR product, single DNA band was observed lying in between 200 and 300bp as indicated by DNA marker when viewed on UV transilluminator. The PCR amplified products were stored at 4°C.
Restriction Digestion of PCR amplified
Products
Steps:
* Incubation at 37°C for 3 hours
* Heat Inactivation at 65°C for 20 minutes
* Holding at 4°C forever.
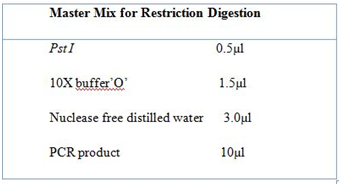
Table3: The reaction mixture for restriction digestion.
Further the incubation of the reaction mixture was carried out in the thermocycler and the following program was used;
Then the digested product was analyzed by agarose gel electrophoresis.
3%Agarose gel Electrophoresis of digested products
After digestion of the 283bp fragment obtained by PCR, to check for three possible genotypes, 15µl of digested products were mixed with 3µl of loading dye and loaded on the wells of 3%agarose gel in 1XTAE buffer along with 100bp DNA ladder for 1 hour at 90 volts. The result was viewed under UV transilluminator for number of DNA fragments obtained.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
RESULT
Genomic DNA was extracted from blood cells. The extracted DNA was run through 1% agarose gel electrophoresis. PCR product was run through 2% agarose gel electrophoresis. Finally digested product was run through 3% agarose gel electrophoresis.
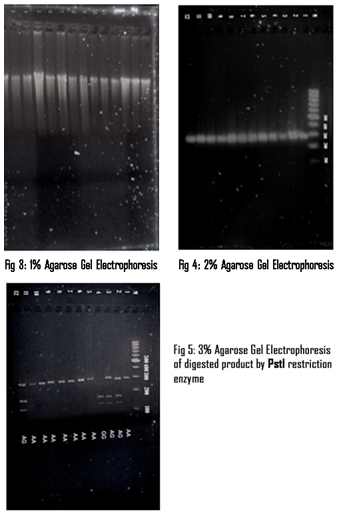
The amplified product was subjected to digestion by PstI restriction enzyme. After digestion of the 283 bp fragment by PCR,165bp,283bp). The restriction enzyme digested fragment was run on 3% agarose gel electrophoresis. The gel picture below depicts the band pattern for genotypes.
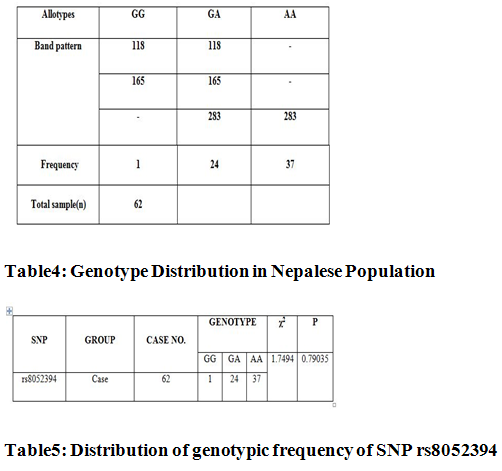
Genotypic distribution was in accordance with Hardy-Weinberg Equilibrium when analysed by PopGene.S2 software with χ2=1.7494, df=1 and P>0.05.
DISCUSSION
The present study revealed an association of MT genes with T2DM. SNP rs8052394 detected in this study was highly polymorphic. The χ2goodness-of-fit test showed that the genotypic distribution of rs8052394 SNP was not deviated from the Hardy- Weinberg equilibrium (P >0.05), suggesting the suitability of this sample pool for genetic analysis. The allelic frequency distribution analysed by PopGene software showed that ‘G’ allele (p=0.79035) is high in Nepalese Population whereas ‘A’ allele (q=0.20965) is less in frequency.
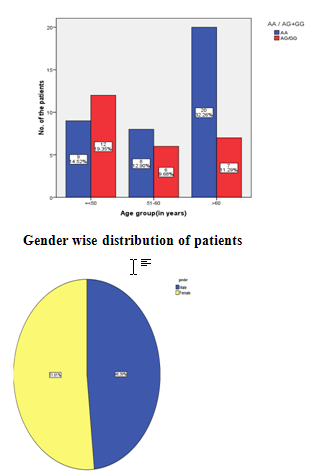
Gender wise distribution of patients
The gender wise distribution of rs8052394 of MT1A gene mutated and wild type or differently mutated strains is presented in Table 7. Among male subjects 30 (48.39%) weresuffering from diabetes and 32(51.61%) were from female subjects. This shows no any significant relationship between the prevalence of diabetes mellitus and gender.
Agewise distribution of the T2DM patient
Agewise distribution of the patient shows that 33.87% people were less than 50 years ,22.58 were between 51-60 and 43.55 %were >61.
|
Age |
<50 |
51-60 |
>61 |
|
Percentage |
33.87 |
22.58 |
43.55 |
|
Total number |
21 |
14 |
27 |
Table6: Agewise distribution in accordance to mutation
In a given diabetic population, the chance of alteration on different genes are possible which are responsible for the induction of T2DM[17][18]..But the role of MT1A is most widely studied due to the importance of this gene. The mutation in MT1A gene is a major mechanism for the development of diabetes and its complications. The most common mutation is the Lys51Arg substitution inMT1A gene, which is present in approximately 36.13% of the diabetic population and is associated with relatively high level induction of the diabetes and its complication [16]. But however it should be remembered that at normal condition MTIA gene acts as antioxidant therefore prevents diabetes[19]. The most frequent mutation patterns of diabetic patient of MT1A gene occurs at rs8052394 fragment at aminoacid51 (36.13%) of MT1Agene. But mutation in MT1A gene occurs in a higher frequency than any other gene and is regarded as to be most important in diagnosing diabetes. [16]
CONCLUSION
The study of genotype frequency distribution for the MT1A polymorphism in rs8052394 in Nepalese population from Nepal for the first time will definitely serve as a major achievement in understanding the molecular level of mechanism and effects of the gene mutation which varies in different geographical region of world.
We found that rs8052394 of MT1A gene mutation at amino acid 51 accounted 40.3% among which the mutation is more commonly found on the age group less than 50years. To the best of our knowledge frequency of the MT1Agene lys51arg mutation has not been previously determined in Nepalese diabetic population. The higher percentage (40.3%) of common mutation in MT1A definitely highlights the importance of the 51st amino acid for development of diabetes and its complication.
BIBLIOGRAPHY
1) World Health Organisation & Department of Non communicable Disease Surveillance (1999). Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications staff.ncl.ac.uk/philip.home/who_dmg.pdf
2) Cooke DW, Plotnick L : Type 1 diabetes mellitus in pediatrics. Pediatr Rev Nov 2008, 29 (11): 374–384.
3) Florence Demenais, Timo Kanninen, Cecilia M. Lindgren, et al .:A meta-analysis of four European genome screens (GIFT Consortium) shows evidence for a novel region on chromosome 17p11.2–q22 linked to type 2 diabetes[abstract]. Human Molecular Genetics 2003, 12(15):1865–1873.
4) Wild S, Roglic G, Green A, Sicree R, King H: Global prevalence of diabetes: estimates for 2000 and projections for 2030. Diabetes Care 2004, 27(5): 1047–1053.
5)Satyanarayana U, Chakrapani U: Biochemistry (3rd edition). Books & Allied (P) Ltd; 2011.
6) Li X, Cai L, Feng W: Diabetes and Metallothionein. Mini Rev Med Chem 2007, 7: 761–768.
7) Carl A. Burtis, Edward R. Ashwood, David E. Bruns: Tietz Textbook of Clinical Chemistry and Molecular Diagnostics(4th edition): Elsevier Health Sciences ; 2005.
8) American diabetes association. Report: Type 2 diabetes in children and adolescents. Diabetes care 2000, 23:381-9
9) The Information Centre (2006). Health Survey for England 2004: Health of ethnic minorities: ic.nhs.uk/statistics-and-data-collections/health-and-lifestyles-related-surveys/health-survey-forengland/health-survey-for-england-2004:-health-of-ethnic-minorities--full-report.
10) Cai L: Diabetic cardiomyopathy and its prevention by metallothionein: experimental evidence, possible mechanisms and clinical implications. Curr Med Chem 2007, 14: 2193–2203.
11) Higashimoto Minoru, Isoyama Naohiro, Ishibashi Satoshi, Inoue Masahisa, Takiguchi Masufumi, Suzuki Shinya, Ohnishi Yoshinari, Sato Masao:Tissue dependent preventive effect of metallothionein against DNA damage in dyslipidemic mice under repeated stresses of fasting or restraint. Life Sciences 2009, 84:569-575
12) J. E. Shaw, R. A. Sicree, and P. Z. Zimmet: Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Research and Clinical Practice 2010, 87(1):4–14.
13) American Diabetes Association. Report: Total Prevalence of Diabetes and Pre-diabetes. diabetes.org/diabetes-statistics/prevalence.jsp
14) Grarup N, Andersen G: Gene-environment interactions in the pathogenesis of type 2 diabetes and metabolism. Current Opinion in Clinical Nutrition & Metabolic Care 2007 10: 420–426.
15) Mikkel Faurschou1, Milena Penkowa2, Claus Bøgelund Andersen3, Henrik Starklint4 and Søren Jacobsen: The renal metallothionein expression profile is altered in human lupus nephritis. Arthritis Research & Therapy 2008, 10:R761
16) Lina yang et al.: Polymorphisms in metallothionein-1 and -2 genes associated with the risk of type 2 diabetes mellitus and its complications. Am J Physiol Endocrinol Metab 2008 294: E987–E992.
17) Shoelson SE, Lee J, Goldfine AB: Inflammation and insulin resistance. J Clin Invest July 2006, 116 (7): 1793–801
18) Lyssenko V, Jonsson A, Almgren P et al. : Clinical risk factors, DNA variants, and the development of type 2 diabetes. The New England Journal of Medicine Nov2008, 359 (21): 2220–2232.
19) Papouli E, Defais M, Larminat F: Over expression of metallothionein-II sensitizes rodent cells to apoptosis induced by DNA cross-linking agent through inhibition of NF-kappaβ activation. J Biol Chem. 2000, 277:4764-4769.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE








