{ DOWNLOAD AS PDF }
 ABOUT AUTHORS
ABOUT AUTHORS
*P.Dhaneshwar1, P.Stephen2, A.N.RAJALAKSHMI1
1* Department of Pharmaceutics,
College of pharmacy,
Mother Theresa Post Graduate & Research Institute Of Health Sciences, Puducherry, India
2 Sai mirra innopharm pvt ltd,
Ambattur, Chennai, India
*dhanesh7pharma@gmail.com
Drug absorption in the gastrointestinal tract is a highly variable process and prolonging gastric retention of the dosage form extends the time for drug absorption. Novel drug delivery system overcomes the physiological problems of short gastric retention through various approaches including floating drug delivery systems (FDDS), these systems float due to bulk density less than gastric fluids and so, remain buoyant in the stomach for a prolonged period of time, releases the drug slowly at the desired rate from the system and increase the bioavailability of narrow absorption window drugs. This review entitles the applications of sustained release effervescent floating bilayer tablets, suitable for sustained release of those drugs incompatible with floating constituents over an extended period of time for better patient compliance and acceptability. The purpose of this paper is to review the principle of sustained release effervescent floating drug delivery system, current technology used in the development of same as well as summarizes the applications, advantages, methodology, evaluation methods and future potential for sustained release effervescent floating bilayer tablets
[adsense:336x280:8701650588]
REFERENCE ID: PHARMATUTOR-ART-2511
|
PharmaTutor (Print-ISSN: 2394 - 6679; e-ISSN: 2347 - 7881) Volume 5, Issue 8 Received On: 04/04/2017; Accepted On: 24/04/2017; Published On: 01/08/2017 How to cite this article: Dhaneshwar P, Stephen P, Rajalakshmi AN;Sustained release effervescent floating bilayer tablets - A review of Novel Approach; PharmaTutor; 2017; 5(8);32-40 |
INTRODUCTION
Oral route is the most convenient and preferred means of drug delivery to the systemic circulation due to its ease of administration, patient compliance, least sterility constraints and flexible design of dosage forms. However, the development process is presented with several physiologic difficulties, such as an inability to restrain and localize the drug delivery system within desired regions of the gastrointestinal tract (GIT), an unpredictable gastric emptying rate that varies from person to person, a brief gastrointestinal transit time and the existence of an absorption window in the upper small intestine for several drugs.
Depending upon the physiological state of the subject and the design of the pharmaceutical formulation, the emptying process can last from a few minutes up to12 hr. This variability, in turn, may lead to unpredictable bioavailability and times to achieve peak plasma levels, since the majority of drugs are preferentially absorbed in the upper part of the small intestine. The relatively brief gastric emptying time (GET) in humans, which normally averages 2 to 3 hr through the major absorption zone (stomach or upper part of the intestine), can result in incomplete drug release from the drug delivery system (DDS) leading to diminished efficacy of the administered dose.
In addition, some drugs display region specific absorption which is related to differential drug solubility and stability in different regions of GIT, as a result of changes in environmental pH, degradation by enzymes present in the lumen of the intestine or interaction with endogenous components such as bile. Active transport mechanisms for drugs involving carriers and pump systems have been also well described. These drugs show absorption window, which signifies the region of GIT where absorption primarily occurs.
Drugs released from sustained/controlled release systems, after absorption window has been crossed, go waste with negligible absorption which indicates that absorption window can limit the bioavailability of orally administered compounds and can be a major obstacle to the development of sustained/controlled release drugs. Therefore, it would be beneficial to develop sustained release formulations which remain at the absorption site for an extended period of time.
One of the feasible approaches for achieving prolonged and predictable drug delivery profile in GIT is to control gastric retention time (GRT) of the formulation. Dosage forms with prolonged GRT, i.e., Gastro Retentive Dosage Forms (GRDFs), will overcome the problems of simple sustained release dosage forms.
Gastro Retentive Dosage Forms (GRDFs)
GRDFs are dosage forms which prolong the retention time of a drug in the GIT, thereby improving the oral bioavailability of the drug.
Over the past three decades, the pursuit and exploration of devices designed to be retained in the upper part of the gastrointestinal (GI) tract has advanced consistently in terms of technology and diversity, encompassing a variety of systems and devices such as floating systems, raft systems, expanding systems, swelling systems, bioadhesive systems and low-density systems.
Gastric retention will provide advantages such as the delivery of drugs with narrow absorption windows in the small intestinal region. Also longer residence time in the stomach could be advantageous for local action in the upper part of the small intestine, for example treatment of peptic ulcer disease. Furthermore, improved bioavailability is expected for drugs that are absorbed readily upon release in the GI tract. These drugs can be delivered ideally by slow release from the stomach.
Many drugs categorized as once-a-day delivery have been demonstrated to have suboptimal absorption due to dependence on the transit time of the dosage form, making traditional extended release development challenging. Therefore, a system designed for longer gastric retention will extend the time within high drug absorption can occur in the small intestine. Certain types of drugs can benefit from using gastric retentive devices. These include:
Drugs acting locally in the stomach: Drugs that are primarily absorbed in the stomach: Drugs those are poorly soluble at an alkaline pH: Drugs with a narrow window of absorption: Drugs absorbed rapidly from the GI tract and Drugs that degrade in the colon.
Basic physiology of the gastrointestinal tract
Anatomically the stomach is divided into three regions: fundus, body, and antrum (pylorus).The proximal part made up of fundus and body acts as a reservoir for undigested material, whereas the antrum is the main site for mixing motions and act as a pump for gastric emptying by propelling actions [Desai S, 1984].
Gastric emptying occurs during fasting as well as fed states. The pattern of motility is however distinct in the two states. During the fasting state an interdigestive series of electrical events take place, which cycle both through stomach and intestine every 2 to 3 hours [Vantrappen GR et al, 1979]. This is called the interdigestive myloelectric cycle or migrating myloelectric cycle (MMC), which is further divided into following 4 phases [Wilson CG et al, 1989].
A. Phase I (basal phase) lasts from 40 to 60 min with rare contractions
B. Phase II (preburst phase) lasts for 40 to 60 minutes with intermittent action potential and contractions. As the phase progresses the intensity and frequency also increases gradually.
C. Phase III (burst phase) lasts for 4 to 6 minutes. It includes intense and regular contractions for short period. It is due to this wave that all the undigested material is swept out of the stomach down to the small intestine. It is also known as the housekeeper wave.
D. Phase IV lasts for 0 to 5 minutes and occurs between phases III and I of 2 consecutive cycles.
After the ingestion of a mixed meal, the pattern of contractions changes from fasted to that of fed state. This is also known as digestive motility pattern and comprises continuous contractions as in phase II of fasted state. These contractions result in reducing the size of food particles (to less than 1 mm), which are propelled toward the pylorus in a suspension form. During the fed state onset of MMC is delayed resulting in slowdown of gastric emptying rate (Bolton S et al, 1989).
Under physiological condition, the gastric absorption of most drugs is insignificant as a result of its limited surface area (0.1 - 0.2 m2) covered by a thick layer of mucous coating, the lack of villi on the mucosal surface, and the short residence time of most drug in the stomach. Rapid gastric emptying, also called dumping syndrome, occurs when undigested food empties too quickly into the small intestine. Stomach emptying is a coordinated function by intense peristaltic contractions in the antrum.
At the same time, the emptying is opposed by varying degrees of resistance to passage of chyme at the pylorus. The rate depends on pressure generated by antrum against pylorus resistance.
Factors affecting gastric retention
1. Density
The density of a dosage form also affects the gastric emptying rate. A buoyant dosage form having a density of less than that of the gastric fluids (1.004 gm/ml) floats.
2. Size and shape
To pass through the pyloric valve into the small intestine the particle size should be in the range of 1 to 2 mm (Wilson CG and Washington N, 1989). Dosage form unit with a diameter of more than 7.5 mm are reported to have an increased GRT compared to those with a diameter of 9.9 mm. The dosage form with a shape tetrahedron and ring shape devices with a flexural modulus of 48 and 22.5 kilopond per square inch (KSI) are reported to have better GIT (90 to 100 %) retention at 24 hours compared with other shapes.
3. Fasting or fed state
Under fasting conditions, the GI motility is characterized by periods of strong motor activity or the Migrating Myoelectric Cycles (MMC) that occurs every 1.5 to 2 hours. The MMC sweeps undigested material from the stomach and if the timing of administration of the formulation coincides with that of the MMC, the GRT of the unit can be expected to be very short. However, in the fed state, MMC is delayed and GRT is considerably longer (Talukder R et al, 2004).
The pH of the stomach in fasting state is ~1.5 to 2.0 and in fed state is 2.0 to 6. A large volume of water administered with an oral dosage form raises the pH of stomach contents to 6.0 to 9.0. Stomach doesn’t get time to produce sufficient acid when the liquid empties the stomach; hence generally basic drugs have a better chance of dissolving in fed state than in a fasting state.
Studies have revealed that gastric emptying of a dosage form in the fed state can also be influenced by its size. Small-size tablets leave the stomach during the digestive phase while the large-size tablets are emptied during the housekeeping waves.
4. Nature of the meal
The rate of gastric emptying depends mainly on viscosity, volume, and caloric content of meals. Nutritive density of meals helps determine gastric emptying time. However, increase in acidity and caloric value slows down gastric emptying time. Feeding of indigestible polymers of fatty acid salts can change the motility pattern of the stomach to a fed state, thus decreasing the gastric emptying rate and prolonging the drug release (Xu WL et al; 1991).
5. Effect of liquid, digestible solid and indigestible solid type food
It has been demonstrated using radio labeled technique that there is a difference between gastric emptying times of a liquid, digestible solid, and indigestible solid. It was suggested that the emptying of large (>1 mm) indigestible objects from stomach was dependent upon interdigestive migrating myoelectric cycle. When liquid and digestible solids are present in the stomach, it contracts ~3 to 4 times per minute leading to the movement of the contents through partially opened pylorus. Indigestible solids larger than the pyloric opening are propelled back and several phases of myoelectric activity take place when the pyloric opening increases in size during the housekeeping wave and allows the sweeping of the indigestible solids. Studies have shown that the gastric residence time (GRT) can be significantly increased under the fed conditions since the MMC is delayed.
6. Biological factors
Biological factors such as age, body mass index (BMI), gender, posture and diseased states (Diabetes, Chron’s disease) influence gastric emptying. In the case of elderly persons, gastric emptying is slowed down. Generally females have slower gastric emptying rates than males. GRT can very between supine and upright ambulatory states of the patients [Mojaverian P et al; 1998]. Stress increases gastric emptying rates while depression slows it down.
7. Frequency of feed
The gastro retentive time can increase by over 400 minutes when successive meals are given compared with a single meal due to the low frequency of MMC [Jain NK, 2004].
8. Gender
Mean ambulatory GRT in meals (3.4 hours) is less compared with their age and race-matched female counterparts (4.6 hours), regardless of the weight, height and body surface.
9. Volume of liquids
The resting volume of the stomach is 25 to 50 ml. Volume of liquids administered affects the gastric emptying time. When volume is large, the emptying is faster. Fluids taken at body temperature leave the stomach faster than colder or warmer fluids.
10. Effect of size of floating and non floating dosage
The effect of size of floating and non floating dosage forms were studied on gastric emptying and concluded that the floating units remained buoyant on gastric fluids. These are less likely to be expelled from the stomach compared with the non floating units, which lie in the antrum region and are propelled by the peristaltic waves. (Timmermans J and Andre JM, 1994)
Gastric emptying and problems
Major adversity encountered through the oral route is the first pass effect, which leads to reduce systematic availability of a large number of a drug. These problems can be exacerbated by alteration in the gastric emptying that occur due to factors such as age, race, sex and disease states, as they may seriously affect the release of a drug from DDS. It is therefore desirable to have a Controlled release product that exhibits an extended, GI residence and a drug release profile independent of patient related variables.
Requirement of Gastric retention
From the discussion of the physiological factors in the stomach, it must be noted that, to achieve gastric retention, the dosage form must satisfy certain requirements. One of the key issues is that the dosage form must be able to withstand the forces caused by peristaltic waves in the stomach and the constant contractions and grinding and churning mechanisms. To function as a gastric retention device, it must resist premature gastric emptying. Furthermore, once its purpose has been served, the device should be removed from the stomach with eases.
Drug candidates for gastric retention
Various drugs have their greatest therapeutic effect when released in the stomach, particularly when the release is prolonged in a continuous and controlled manner.
Potential drug candidates for gastroretentive drug delivery systems include: drugs that are locally active in the stomach (e.g. misoprostol, antacids etc.); drugs that have narrow absorption window in gastrointestinal tract (e.g. L-DOPA, Para-aminobenzoic acid, Furosemide, Riboflavin, Salbutamol [Swarbrick, 2007; Shinde et al, 2010]); drugs that are unstable in the intestinal or colonic environment (e.g. captopril, ranitidine HCl, metronidazole.); drugs that disturb normal colonic microbes (e.g. antibiotics against Helicobacter pylori) and drugs that exhibit low solubility at high pH values (e.g. diazepam, chlordiazepoxide, verapamil HCl).
Approaches for gastric retention
Hydro dynamically balanced systems (HBS) –incorporated buoyant materials enable the device to float. Raft systems incorporate alginate gels – these have a carbonate component and, upon reaction with gastric acid, bubbles form in the gel, enabling floating [Whitehead L et al, 1996; Iannuccelli V et al; 1998].
Swelling type of dosage form is such that after swelling, this product swells to extent that prevents their exit from the stomach through the pylorus. As a result, the dosage form retained in the stomach for a longer period of time. These systems may be referred to as a “Plug type system”, since they exhibit tendency to remain logged in the pyloric sphincters (Bolton S et al, 1989).
Bioadhesive or mucoadhesive systems are used to localize a delivery device within the lumen and cavity of the body to enhance the drug absorption process in a site - specific manner. The approaches involve the use of bioadhesive polymers that can be adhered to the epithelial surface of the GIT. The proposed mechanisms of bioadhesive are the formation of hydrogen and electrostatic bonding at the mucus polymer boundary [Jimenez-Castellanos NR et al, 1993].
Modified shape systems are non-disintegrating geometric shapes molded from silastic elastomer or extruded from polyethylene blends and extended the GET depending on the size, shape and flexural modulus of the drug delivery device.
High-density formulations include coated pallets, and have density greater than that of the stomach content (1.004 gm/cm3). This is accomplishing by coating the drug with a heavy inert material such as barium sulphate, ZnO, titanium dioxide. This formulation of high-density pellet is based on assumption that heavy pellets might remain longer in the stomach, since they are position in the lower part of the antrum [Talukder R et al, 200]).
Another delayed gastric emptying approach of interest include sham feeding of digestible polymers or fatty acid salts that charges the motility pattern, of the stomach to a fed stage thereby decreasing the gastric emptying rate and permitting considerable prolongation of the drug release.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
FLOATING DRUG DELIVERY SYSTEM
Floating drug delivery systems have a bulk density less than gastric fluids and so remain buoyant in the stomach without affecting the gastric emptying rate for a prolonged period of time. While the system is floating on the gastric contents, the drug is released slowly at the desired rate reliably buoyant on the surface of the meal. Many buoyant systems have been developed based on granules, powders, capsules, tablets, laminated films and hollow microspheres. Floatation of drug delivery system in the drug can be achieved by incorporating floating chamber filled with vacuum, air or inert gas from the system. After release of drug, the residual system is emptied from the stomach. This results in an increased GRT and a better control of fluctuations in plasma drug concentration. However, besides a minimal gastric content needed to allow the proper achievement of the buoyancy retention principle, a minimal level of floating force is also require to keep the dosage form.
Types of Floating Drug Delivery Systems
Based on the mechanism of buoyancy, two distinctly different technologies have been utilized in the development of FDDS.
A. Effervescent system
a. Volatile liquid containing system
b. Gas generating system
B. Non-effervescent system
a) Alginate beads
b) Hollow microspheres
c) Single layer floating tablets
d) Bilayer floating tablets
e) Colloidal gel barrier system
f) Microporous compartment system
A. Effervescent FDDS
a) Volatile liquid containing system: The GRT of a drug delivery system can be sustained by incorporating an inflatable chamber, which contains a liquid e.g. ether, cyclopentane, that gasifies at body temperature to cause the inflatation of the chamber in the stomach. The device may also consist of a bioerodible plug made up of Polyvinyl alcohol, Polyethylene etc. that gradually dissolves causing the inflatable chamber to release gas and collapse after a predetermined time to permit the spontaneous ejection of the inflatable systems from the stomach11.
b) Gas-generating Systems: These buoyant delivery systems utilize effervescent reactions between carbonate/bicarbonate salts and citric/tartaric acid to liberate CO2, which gets entrapped in the jellified hydrocolloid layer of the systems thus decreasing its specific gravity and making it to float over gastric content.
SUSTAINED RELEASE EFFERVESCENT FLOATING BILAYER TABLETS
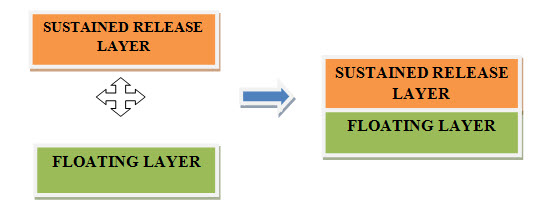
Sustained release effervescent floating bilayer tablets is composed of two layers. A layer of sustained release polymer and drug (Sustained release layer) and a layer of effervescent floating components (Floating layer). Such a formulation offers more advantages compared to single layer effervescent floating tablets in terms of stability. Since effervescent components are unstable and incompatible with many potential drug candidates for gastric retention such a approach could be highly beneficial.
Advantages of sustained release bilayer floating tablets
1. This system provides sustained delivery of drugs along with enhanced gastric residence time as this system remains in stomach for many hours via floating.
2. This system finds additional advantages over single layer floating drug delivery system in terms of stability of the formulation.
3. Better patient compliance is achieved due to its ease of administration.
4. It maintains constant blood level.
5. Site specific drug delivery is achieved for the drugs such as Furosemide and Riboflavin which are formulated as floating system.
6. Over all other oral routes these are microbiologically and chemically stable.
7. Due to higher dose precision and lesser content variation they are the most compatible oral dosage form.
8. They offer the most flexible dosage form.
9. Better suited for large scale production.
Methodology used for bilayer floating tablets [Pujar ND et al.,2012]
1. Oros ® Push Pull Technology
2. L-Oros Tm Technology
3. DUROS Technology
4. Elan Drug Technologies’ Dual Release Drug Delivery System
5. EN SO TROL Technology
6. Rotab Bilayer
7. Geminex Technology
1. Oros ® Push Pull Technology: Two or three layer system a drug layer and push layer. Drug layer contain drug with other agents and due to this drug is less soluble. Sometimes suspending agent and osmotic agent are also added. The tablet core is surrounded by semi permeable membrane.
2. L-Oros Tm Technology: Alza developed L-OROS system due to solubility problem. The system contain a drug in dissolved state in a lipid soft gel product which is produced first and then barrier membrane, after which osmotic membrane and semi permeable membrane coat is applied and is then drilled out through external orifice.
3. DUROS Technology: This technology is also known as miniature drug dispensing system which works like a miniature syringe and release small quantity of drug consistently over a period of time .There is an outer cylindrical titanium alloy reservoir which has high impact strength due to which drug molecules inside it are protected from enzymes.
4. Elan Drug Technologies’ Dual Release Drug Delivery System: The DUREDASTM Technology provides combination release of drugs together and different release pattern of single drug i.e. it provides sustained release as well as immediate release. This technology provides various advantages i.e. two drug components provide tailored release and its another benefit is that it consist of bilayered tablet technology in which it contain modified as well as immediate release pattern in one tablet. In these different controlled release formulations are combined together.
5. EN SO TROL Technology: An integrated approach is used by Shire laboratory for drug delivery system which focus on identification and incorporation of enhancer which is identified to form optimized dosage form in controlled release system. By this enhancement in solubility is achieved.
6. RoTab Bilayer: RoTab bilayer when using is switched to production mode. Dose and compression force is automatically regulated by adjusting filling speed and die table. Hardness is also regulated when required.
7. Geminex Technology: In this drug delivery system at different times more than one drug can be delivered. This technology basically increases the therapeutic efficacy of the drug by decreasing its side effects. It is useful both to industry as well as patient as in single tablet it provides delivery of drug at different rates.
Characterization of bilayer floating tablets [Dixit N.2011]
In-vitro evaluation of floating tablets Evaluation was performed to assess the physicochemical properties and release characteristics of the developed formulations.
Pre-compression parameters
Angle of Repose
In powder, frictional forces can be measured with the help of angle of repose. Angle of repose is the maximum angle which is possible between surface of pile of powder and horizontal plane i.e. height.
tanΘ= h/r Θ=tan-1h/r
Where Θ = Angle of repose, h= height of pile, r = radius of pile.
Compressibility Index
The propensity of the powder to be compressed is measured by compressibility index and it also helps in measurement of settling property and interparticulate interaction.
Compressibility index (%) = ρt – ρo* 100 / ρt
Where ρt = Tapped density gram/ml, ρo = Bulk density gram/ml.
Bulk Density
It is denoted by ρb and is defined as mass of powder divided by bulk volume (The United States Pharmacopeial Convention Stage 6 Harmonization Official December 1, 2012, 616.).
Tapped Density
An increase in bulk density which is attained after mechanical tapping in measuring cylinder is called as tapped density.
Tapped density= Weight of powder taken/ Tapped Volume
Hausner Ratio
The propensity of the powder to be compressed is measured by Hausner ratio. Interparticulate interaction and settling property can be measured by Hausner ratio.
Hausner ratio= Tapped density/ Bulk density Hausner ratio= Vo/Vf
Where, Vo= Unsettled apparent volume, Vf= Final tapped volume.
Particle Size Distribution
Particle size distribution was done by sieving method.
Post-compression parameters
Tablet Thickness
In this three tablets are randomly taken and then their thickness and diameter are measured by Vernier calliper or by using calibrated screw gauze.
Weight Variation Test
Twenty tablets are selected and weighed individually. Then the average weight and standard deviation is calculated. Test passes when not more than two tablets deviate from average weight.
Hardness
Expressed in kg/cm2 and it is checked using Monsanto hardness tester by randomly picking three tablets. Hardness helps in knowing ability of the tablet to withstand mechanical shock during handling of tablets.
Friability
Ten tablets are selected and weighed and then placed in friabilator apparatus which rotate at 25 rpm speed for 4 minutes. After 4 minutes tablets are weighed again.
% F= [1-(Wt/W)]*100
where
W– Initial weight of tablet, Wt - Weight of tablet after revolution. If % Friability of tablets is less than 1% is considered acceptable.
Tablet Density t is an important parameter in case of floating tablets. If density is less than (1.004) gastric fluid, than only the tablets will float. It is calculated using formula:
V=πr2h, d = m/v,
r = Radius of tablet, h = crown thickness (g/cc), m = Mass of tablet.
Disintegration Time
In this one tablet is placed in disintegration apparatus containing buffer 0.1N Hcl or PBS pH 6.8 and test is carried out at 37oC. The time taken by tablet to Disintegrate is noted as disintegration time.
In Vitro Dissolution Studies Dissolution study is performed using USP paddle apparatus by maintaining optimum temperature i.e., 370C at 50 rpm rotational speed. At various time interval 5 ml sample is withdrawn and is replaced with same amount of buffer.
Floating Lag Time
It is the time interval taken by the tablets to start floating. It should be less than one minute. It is measured by dissolution test apparatus containing 0.1 N Hcl (900ml).
Floating Time
It is the total time taken by which the tablets remain floating in the media.
Drug Content Uniformity
Ten tablets are taken and powdered equivalent weight of drug dose is taken and is transferred to volumetric flask and then buffer is added and absorbance is determined using U.V spectrophotometer.
Swelling Study
Initially tablet is weighed (W1) and placed in a glass beaker, containing 200 mL of 0.1 N HCl, maintained in a water bath at 37 ± 0.5 _C. At different time intervals, the tablet is removed and the excess of liquid is carefully removed by a filter paper. The swollen tablet is reweighed (W2). The swelling index (SI) is calculated using the formula
SI= Wt -W0/W0*100
Wt= (Weight of swollen tablet), W0= (Initial weight of tablet).
In-vivo evaluation
a) Radiology
X-ray is widely used for examination of internal body systems. Barium Sulphate is widely used Radio Opaque Marker. So, BaSO4 is incorporated inside dosage form and X-ray images are taken at various intervals to view gastric retention.
b) Scintigraphy
Similar to X-ray, emitting materials are incorporated into dosage form and then images are taken by scintigraphy. Widely used emitting material is 99Tc.
c) Gastroscopy
Gastroscopy is peroral endoscopy used with fiber optics or video systems. Gastroscopy is used o inspect visually the effect of prolongation in stomach. It can also give the detailed evaluation of GRDDS.
d) Magnetic Marker Monitoring
In this technique, dosage form is magnetically marked with incorporating iron powder inside, and images can be taken by very sensitive bio-magnetic measurement equipment. Advantage of this method is that it is radiation less and so not hazardous.
e) Ultrasonography
Used sometimes, not used generally because it is not traceable at intestine. f) 13C Octanoic Acid Breath Test
13C Octanoic acid is incorporated into GRDDS. In stomach due to chemical reaction, octanoic acid liberates CO2 gas which comes out in breath. The important Carbon atom which will come in CO2 is replaced with 13C isotope. So time up to which 13CO2 gas is observed in breath can be considered as gastric retention time of dosage form. As the dosage form moves to intestine, there is no reaction and no CO2 release. So this method is cheaper than other.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Future potential for sustained release bilayer floating tablets
Drug release is the major area in the pharmaceutical research work. Through sustained release bilayer floating tablets release can be increased up to 24 hours for drugs incompatible with effervescent floating components, hence this system finds greater advantages over single layer effervescent floating tablets in terms of stability. It is also beneficial in providing gastric retention thereby increasing gastric emptying time as well as increasing bioavailability and reducing dosing frequency which provides better patient compliance. It provides a great opportunity in case of herbal drugs as these drugs can also be given in sustained release effervescent floating bilayer dosage form which provides greater stability to the formulation. Drugs having narrow absorption window such as anti-viral, antibiotic and antifungal can also be given in sustained release floating bilayer dosage form.
REFERENCES:
1) Bolton S, Desai S; Floating sustained release therapeutic compositions; US Patent; 4, 814, 179; March 21; 1989.
2) Desai S.A; Novel Floating controlled release drug delivery system based on a dried gel matrix Network (master’s thesis) Jamaica; NY: St. John’s University; 1984.
3) Dixit N. Floating Drug Delivery System. J Current Pharm Res. 2011;7(1):6-20.
4) Jain N K; Progress in controlled and novel drug delivery systems, First Ed.; 2004,CBS Publishers and Distributors; New Delhi; Bangalore: 84-85.
5) Jimenez-Castellanous N.R, Zia H and Rhodes C.T; Mucoadhesive drug delivery Systems; Drug Development and Industrial Pharmacy; 1993; 19; 143.
6) Mojaverian P, Ferguson R.K, Vlasses P.H; Estimation of gastric residence time of the heidelberg capsules in humans: effect of varying food composition; Scandinavian journal of Gastroenterology; 1985; 89; 392-397.
7) Pujar ND, Gokani RK, Paun JS. Bilayer Tablet – An Emerging Trend. International Journal of Pharmaceutical Research and Development. 2012, 4, 102 – 111.
8) Talukder R and Fissihi R; Gastroretentive delivery systems: A mini review; Drug Development & Industrial pharmacy; 2004; 30(10); 1019-1028.
9) Timmermans J, Andre J.M; Factors controlling the buoyancy and gastric retention capabilities of floating matrix capsules: new data for reconsidering the controversy; Journal of Pharmaceutical science; 1994; 83; 18-24.
10) Vantrappen G.R, Peeters T.L, Janssens J; The secretory component of interdigestive migratory motor complex in man; Journal of Gastroenterology; 1979; 14;663-667.
11) Whitehead L, Fell J.T, Collett J.H; Development of a gastroretentive dosage form; European Journal of Pharmaceutical Sciences; 1996; 4(1); 182.
12) Wilson C.G, Washington N; The stomach: its role in oral drug delivery. In: physiological pharmaceutical biological barriers to drug absorption. Chichester, UK: Ellis Horwood; 1989; 47-70.
13) Xu W.L, Tu X.D, Lu Z.D; Develpoment of Gentamycin sulfate sustained release tablets remaining-floating in stomach; AAPS Pharm Tech;1991; 26(7); 541-545.
14) Yang L, Eshraghi J, Fassihi R; A new intragasrtic delivery system for the treatment of Helicobacter pylori associated gastric ulcer: in vitro evaluation; Journal of Controlled Release; 1989; 57;215-222.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE