
About Authors:
Rahul .S.Marathe* , Prof.Mrs.M.S.Patil
A.R.Ajmera College Of Pharmacy,
Nagaon, Dhule (MS)
*rahulmarathe605@gmail.com
Abstract:
Attention deficit hyperactivity disorder (ADHD) is one of the most common childhood disorders and can continue through adolescence and adulthood. Symptoms include difficulty staying focused and paying attention, difficulty controlling behavior, and hyperactivity (over activity). The disorder is commonly occurred in 3 to 7 out of every 100 school-aged children. ADHD is commonly perceived as a childhood disorder, but it persists into adulthood in 35% to 70% of affected people.
Symptoms occur at an early age, occur in most areas of a child’s life, and persist over time, frequently into adulthood The precise constellation of symptoms changes as children grow and develop.With proper medication and handling the child can grow up to be a vibrant, active and successful adult. Not all children and youth havethe same type of ADHD. Some may be hyperactive. Others maybe under-active. Some may have great problems with attention. Others may be mildly inattentive but overly impulsive.
REFERENCE ID: PHARMATUTOR-ART-1753
Introduction:
ADHD is a heterogeneous disorder with many known causes, all of which mediate similar or identical effects on brain functioning.Until recently (ADHD) was perceived as primarily a disease of childhood. Thus, diagnostic criteria and guidelines for the assessment, diagnosis, and treatment of ADHD in children are well established
There are three subtypes of ADHD:
A. Predominantly Inattentive Type
B. Predominantly Hyperactive-Impulsive Type
C. Combined Type (inattention,hyperactivity-impulsivity) fidgety, or impulsive.
Causes:
Scientists are not sure what causes ADHD, although many studies suggest that genes play a large role. Like many other illnesses, ADHD probably results from a combination of factors. In addition to genetics, researchers are looking at possible environmental factors, and are studying how brain injuries, nutrition, and the social environment might contribute to ADHD.
Genes-- Inherited from our parents, genes are the "blueprints" for who we are. Results from several international studies of twins show that ADHD often runs in families. Researchers are looking at several genes that may make people more likely to develop the disorder. Knowing the genes involved may one day help researchers prevent the disorder before symptoms develop. Learning about specific genes could also lead to better treatments
Children with ADHD who carry a particular version of a certain gene have thinner brain tissue in the areas of the brain associated with attention. This NIMH research showed that the difference was not permanent, however, and as children with this gene grew up, the brain developed to a normal level of thickness. Their ADHD symptoms also improved.
Environmental factors- Studies suggest a potential link between cigarette smoking and alcohol use during pregnancy and ADHD in children. In addition, preschoolers who are exposed to high levels of lead, which can sometimes be found in plumbing fixtures or paint in old buildings, may have a higher risk of developing ADHD.
Brain injuries- Children who have suffered a brain injury may show some behaviors similar to those of ADHD. However, only a small percentage of children with ADHD have suffered a traumatic brain injury.
Sugar- The idea that refined sugar causes ADHD or makes symptoms worse is popular, but more research discounts this theory than supports it. In one study, researchers gave children foods containing either sugar or a sugar substitute every other day. The children who received sugar showed no different behavior or learning capabilities than those who received the sugar substitute. Another study in which children were given higher than average amounts of sugar or sugar substitutes showed similar results.
In another study, children who were considered sugar-sensitive by their mothers were given the sugar substitute aspartame, also known as Nutrasweet. Although all the children got aspartame, half their mothers were told their children were given sugar, and the other half were told their children were given aspartame. The mothers who thought their children had gotten sugar rated them as more hyperactive than the other children and were more critical of their behavior, compared to mothers who thought their children received aspartame.
Food additives- Recent British research indicates a possible link between consumption of certain food additives like artificial colors or preservatives, and an increase in activity. Research is under way to confirm the findings and to learn more about how food additives may affect hyperactivity.
Symptoms:
Symptoms of inattention:
- Failing to pay close attention to details or making careless mistakes in schoolwork or other activities
- Trouble sustaining attention during tasks or play
- Not listening even when spoken to directly
- Difficulty following through on instructions resulting in failing to finish schoolwork, or other tasks
- Problems in organizing tasks or activities
- Avoidance of tasks that require sustained attention, such as schoolwork or homework
- Often forgetful and frequently losing needed items, such as books, pencils, toys or tools
- easily distracted by extraneous stimuli;
- is often forgetful in daily activities.
Symptoms of hyperactivity & impulsivity:
- Fidgeting or squirming frequently and leaving the seat in situations when remaining seated is expected (e.g. classroom)
- Constantly on the go running or climbing excessively when it's not appropriate
- Inability to play quietly
- Talking excessively and blurts out replies before questions have been completely asked and interrupting or intruding on others' conversations or games
- Difficulty waiting for their turn
- often fidgets with hands or feet or squirms in seat;
- often leaves seat in classroom or in other situations in which remaining seated is expected;
- is often “on the go” or often acts as if “driven by a motor;”
- often talks excessively.
Pathophysiology
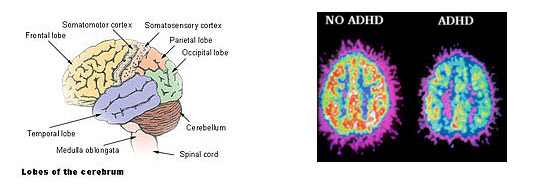
The Pathophysiology of ADHD is unclear and there are a number of competing theories. Research on children with ADHD has shown a general reduction of brain volume, but with a proportionally greater reduction in the volume of the left-sided prefrontal cortex. These findings suggest that the core ADHD features of inattention, hyperactivity, and impulsivity may reflect frontal lobe dysfunction, but other brain regions in particular the cerebellum have also been implicated. Neuroimaging studies in ADHD have not always given consistent results and as of 2008 are used only for research and not diagnostic purposes. A 2005 review of published studies involving neuroimaging, neuropsychological genetics, and neurochemistry found converging lines of evidence to suggest that four connected frontostriatal regions play a role in the pathophysiology of ADHD: The lateral prefrontal cortex, dorsal anterior cingulate cortex, caudate, and putamen.
It should be noted that stimulant medication itself may affect growth factors of the central nervous system.
The same laboratory had previously found involvement of the "7-repeat" variant of the dopamine D4 receptor gene, which accounts for about 30 percent of the genetic risk for ADHD, in unusual thinness of the cortex of the right side of the brain; however, in contrast to other variants of the gene found in ADHD patients, the region normalized in thickness during the teen years in these children, coinciding with clinical improvement.
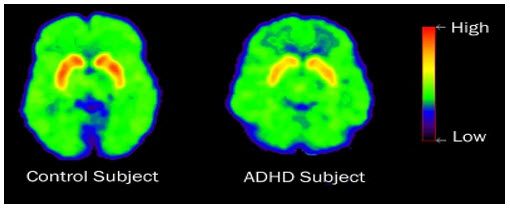
Previously it was thought that the elevated number of dopamine transporters seen in ADHD patients was part of the pathophysiology of ADHD but it now appears that the reason for elevated striatal dopamine transporter density in ADHD individuals is due to neuroadaptations occurring due to the continuous exposure to stimulants such as methylphenidate or dexamphetamine as the body tries to counter-act the effects of the stimulants by developing a tolerance to the stimulant medications. One interpretation of dopamine pathway tracers is that the biochemical "reward" mechanism works for those with ADHD only when the task performed is inherently motivating; low levels of dopamine raise the threshold at which someone can maintain focus on a task that is otherwise boring. There is evidence that people with ADHD have a low arousal threshold and compensate for this with increased stimuli, which in turn results in disruption of attentional capacity and an increase in hyperactive behaviour. The reason for this is due to abnormalities in how the dopamine system in central nervous system responds to stimuli.
Critics, such as Jonathan Leo and David Cohen, who reject the characterization of ADHD as a disorder, contend that the controls for stimulant medication usage were inadequate in some lobar volumetric studies, which makes it impossible to determine whether ADHD itself or psychotropic medication used to treat ADHD is responsible for the decreased thickness observed in certain brain regions. While the main study in question used age-matched controls, it did not provide information on height and weight of the subjects. These variables it has been argued could account for the regional brain size differences rather than ADHD itself. They believe many neuroimaging studies are oversimplified in both popular and scientific discourse and given undue weight despite deficiencies in experimental methodology.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Diagnosis:
ADHD is considered a mental health disorder. Only a licensed professional, such as a pediatrician, psychologist, neurologist, psychiatrist, or clinical social worker, can make the diagnosis that a child, teen, or adult has ADHD. In order to be diagnosed with ADHD, children and youth must meet the specific diagnostic criteria These criteria are primarily associated with the main features of the disability: inattention, hyperactivity, and impulsivity.
The American Academy of Pediatrics (2000) recommends that clinicians collect the following information when evaluating a child for ADHD:
1. A thorough medical and family history.
2. A medical examination for general health and neurologic status.
3. A comprehensive interview with the parents, teachers, and child.
4. Standardized behavior rating scales, including ADHD-specific ones completed by parents, teacher(s), and the child when
Condition associated with ADHD:
Oppositional Defiant Disorder (ODD)—A pattern of negative, hostile, and defiant behavior. Symptoms include frequent loss of temper, arguing (especially with adults), refusal to obey rules, intentionally annoying others, blaming others. The person is angry, resentful, possibly spiteful, and touchy. (Many of these symptoms disappear with ADHD treatments.)
Conduct Disorder (CD)—A pattern of behavior that persistently violates the basic rights of others or society’s rules. Behaviors may include aggression toward people and animals, destruction of property, deceitfulness or theft, or serious rule violations.
Anxiety— Excessive worry that occurs frequently and is difficult to control. Symptoms include feeling restless or on edge, easily fatigued, difficulty concentrating, irritability, muscle tension, and sleep disturbances.
Depression— A condition marked by trouble concentrating, sleeping, and feelings of dejection and guilt. There are many types of depression. With ADHD you might commonly see dysthymia, which consists of a depressed mood for many days, over or under eating, sleeping too much or too little, low energy, low self-esteem, poor concentration, and feeling hopeless. Other forms of depression may also be present.
Learning Disabilities— Problems with reading, writing, or mathematics. When given standardized tests, the student’s ability or intelligence is substantially higher than his or her achievement. Underachievement is generally considered age-inappropriate.
Treatment:
Standard treatments for ADHD in children include medications and counseling. Other treatments to ease ADHD symptoms include special accommodations in the classroom, and family and community support.
Like many medical conditions, ADHD is managed, not cured. There’s no “quick fix” that resolvesthe symptoms of the disorder. Yet a lot can be done to help. Through effective management, some of thesecondary problems that often arise out of untreated ADHD may be avoided. In the majority of cases, AD/HD management will be a lifelong endeavor. It may be helpful to think of AD/HD as a challenge thatcan be met. Recently, the National Institute of Mental Health (NIMH), in combination with the U.S. Department of Education’s Office of Special Education Programs (OSEP), completed a long-term, multi-site study to determine which treatments had the greatest positive effect on reducing AD/HD symptoms. This study is known as the MTA study MTA stands for multimodal treatment study of children with AD/HD.
The recommended multi-modal treatment approach consists of four core interventions:
1. patient, parent, and teacher education about the disorder;
2. medication (usually from the class of drugs called stimulants);
3. behavioral therapy; and
4. other environmental supports, including an appropriate school program.
Pharmacological Treatment:
Stimulants are the first line of treatment for ADHD Stimulants, including methylphenidate and amphetamines, have been widely and successfully used in children for decades. Current pediatric guidelines recommend them as first-line therapy Fewer controlled trials of stimulants have been conducted in adults than in children but results of such studies in adults are similar to those in children and adolescents Controlled trials in adults report significantly greater improvements with stimulants than with placebo, and response rates of 54% to 78% are seen using standard rating scales
Nonpharmacological Treatment :
In addition to pharmacotherapy, nonpharmacologic interventions, such as helping the patient restructure their environment, develop organizational skills, and create better coping strategies, may be beneficial in adults with ADHD Because ADHD affects the entire family, treatment interventions may involve the spouse and children in restructuring of task sharing, planning, and day-to-day functioning. Cognitive-behavioral psychotherapy and structured problem-solving and coping-skills training for ADHD may also improve residual deficits and symptoms that may persist in spite of medication therapy
Medication :
The MTA study found medication to be very effective in the management of AD/HD symptoms. Since AD/HD is a neuro-biochemically- based problem, it stands to reason that medication that gets to the core of the problem would be effective. The medication most often used is stimulant medication, especially methylphenidate. Most people know this medication as the drug Ritalin.
other stimulant medications— Concerta, Metadate, Dexedrine, Cylert, and Adderall, an amphetamine compound. These medications are believed to work by stimulating the action of the brain’s neurotransmitters, especially dopamine. With the brain’s systems working more efficiently, attention, memory, and executive functions, including inhibition, are improved. The result is better concentration, increased working memory capacity, greater recall, less hyperactivity, and more impulse control. Stimulant medications do not tend to help with symptoms of anxiety or depression
Do medications cure ADHD?
Current medications do not cure ADHD. Rather, they control the symptoms for as long as they are taken. Medications can help a child pay attention and complete schoolwork. It is not clear, however, whether medications can help children learn or improve their academic skills. Adding behavioral therapy, counseling, and practical support can help children with ADHD and their families to better cope with everyday problems. Research funded by the National Institute of Mental Health (NIMH) has shown that medication works best when treatment is regularly monitored by the prescribing doctor and the dose is adjusted based on the child's needs.
Psychotherapy
Different types of psychotherapy are used for ADHD. Behavioral therapy aims to help a child change his or her behavior. It might involve practical assistance, such as help organizing tasks or completing schoolwork, or working through emotionally difficult events. Behavioral therapy also teaches a child how to monitor his or her own behavior. Learning to give oneself praise or rewards for acting in a desired way, such as controlling anger or thinking before acting, is another goal of behavioral therapy. Parents and teachers also can give positive or negative feedback for certain behaviors. In addition, clear rules, chore lists, and other structured routines can help a child control his or her behavior.
Therapists may teach children social skills, such as how to wait their turn, share toys, ask for help, or respond to teasing. Learning to read facial expressions and the tone of voice in others, and how to respond appropriately can also be part of social skills training.
What are the side effects of stimulant medications?
The most commonly reported side effects are decreased appetite, sleep problems, anxiety, and irritability. Some children also report mild stomachaches or headaches. Most side effects are minor and disappear over time or if the dosage level is lowered.
- Decreased appetite. Be sure your child eats healthy meals. If this side effect does not go away, talk to your child's doctor. Also talk to the doctor if you have concerns about your child's growth or weight gain while he or she is taking this medication.
- Sleep problems .If a child cannot fall asleep, the doctor may prescribe a lower dose of the medication or a shorter-acting form. The doctor might also suggest giving the medication earlier in the day, or stopping the afternoon or evening dose. Adding a prescription for a low dose of an antidepressant or a blood pressure medication called clonidine sometimes helps with sleep problems. A consistent sleep routine that includes relaxing elements like warm milk, soft music, or quiet activities in dim light, may also help.
- Less common side effects. A few children develop sudden, repetitive movements or sounds called tics. These tics may or may not be noticeable. Changing the medication dosage may make tics go away. Some children also may have a personality change, such as appearing "flat" or without emotion.
Are stimulant medications safe?
Under medical supervision, stimulant medications are considered safe. Stimulants do not make children with ADHD feel high, although some kids report feeling slightly different or "funny." Although some parents worry that stimulant medications may lead to substance abuse or dependence, there is little evidence of this.
Conclusion:
Adult ADHD remains under-recognized, underdiagnosed, and undertreated by clinicians in the US. Its prevalence and the absence of relevant professional clinical training indicate a need to educate physicians and other healthcare providers who encounter the challenging task of diagnosing ADHD in adults. Updated DSM-IV-TR diagnostic criteria that recognize adult-specific symptoms and reconsider age-threshold criteria for symptom onset are needed. Meanwhile, clinicians can improve patient care and provide a better quality of life for these patients and their families by maintaining a high index of suspicion for ADHD, making screening for the disorder an intrinsic part of the standard psychiatric evaluation, and implementing a multifaceted approach to the diagnosis and treatment of adult ADHD.Stimulants that have been used in the pediatric ADHD population for decades are effective and well tolerated in adults. Management of ADHD in adulthood requires the clinician to rule out fairly common medical conditions, such as hypertension, that may be exacerbated by stimulant treatment. Significant cardiac disease in most cases precludes the use of stimulants in both adults and children. However, risk/benefit assessment and a cardiologic consultation may be necessary when the severity of ADHD leads to severe life impairments. Longer-acting forms of stimulants and nonstimulants can improve convenience and extend control of ADHD symptoms in challenging adult environments and potentially may help decrease, but by no means eliminate, the likelihood of stimulant abuse and diversion. In a recent analysis[18] of US prescribing patterns, long-acting medications were still being used more commonly to treat ADHD in children and adolescents (78%) than in adults (49%), though adults may have even greater problems with treatment adherence and drug abuse and diversion than those ≤18 years of age. Alternative medications offer options to those patients with stimulant intolerance or special clinical circumstances such as active substance abuse.
References:
1)American Academy of Pediatrics. (2000,May). Clinical practice guideline: Diagnosis and evaluation of the child with attention-deficit/ hyperactivity disorder. Pediatrics, 105(5), 1158-1170.
2)American Psychiatric Association. (2000).
3)Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: Author. Barkley, R.A. (2000). Taking charge of ADHD:
4)Barkley, R.A., DuPaul, G., & O’Connor, D. (1999). Stimulants. In J.S. Werry & M.G. Aman (Eds.), Practitioner’s guide to psychoactive drugs for children and adolescents (2nd ed.). New York: Plenum.
5)MTA Cooperative Group. (1999, December). A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 56(12), 1073-1086.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE








