{ DOWNLOAD AS PDF }
ABOUT AUTHOR
Senthamil Selvan T *
Pharmaceutical Technical service department,
Mylan Laboratories Limited, Tamilnadu, India
Pharmtamil@gmail.com
ABSTRACT
Dementia is a chronic progressive disorder mainly causes the memory loss and cognitive dysfunction due to neurodegeneration. It is popularly known as Alzheimer disease. It is the fifth disorder leads to death. Those who are the people have crossed age 60 years risk chance of cause. Dementia the disorder is widely known as Alzheimer’s disease, senile dementia, vascular Dementia, Dementia with levy bodies, Parkinson’s disease, Frontotemporal dementia. By neurological examination like CT, MRI, and Spinal fluid analysis can occasionally be justified to confirm the dementia syndrome. For the AD the treatment are broadly takes place as two types, one is cognitive symptoms treatment, another Non- cognitive symptoms treatment. In that case for cognitive sign treatment cholinesterase inhibitors (such as Donepezil, rivastigmine), NMDA receptor inhibitors (Memantine) are used. Anti-psychotics’, Anti-depressant category drugs are used for Non-cognitive symptoms treatment.
[adsense:336x280:8701650588]
Reference Id: PHARMATUTOR-ART-2541
|
PharmaTutor (Print-ISSN: 2394 - 6679; e-ISSN: 2347 - 7881) Volume 5, Issue 11 Received On: 02/08/2017; Accepted On: 02/08/2017; Published On: 01/11/2017 How to cite this article: Senthamil ST; A review approach of Alzheimer Disease and Pharmacological Management; PharmaTutor; 2017; 5(11); 53-57 |
INTRODUCTION
Dementia is a chronic progressive clinical condition of neurodegenerative disease characterized by the memory loss and reduction of cognitive function. Dementia is neurologic disease of the brain leading to the irreversible loss of neurons and the loss of intellectual abilities.(1) Although neurodegeneration is the most common cause, trauma, ischemia, depression, or substance abuse are also possible causes to lead AD.(2) In the year of 2050 1 in 5 people will cross the age 65 years the risk is chance of cause AD In the year of 2001 census shown the population of India indicate the aged peoples accounted as 77 million when compared to 1961 it is 5.63% more. In the year of 2001 it crosses the 7.5%. Both the prevalence and incidence of dementia related exponentially with age to increase level. In 2010, estimation of census indicates 35.6 million people worldwide lived with dementia; around 8 million newer dementia patients are appeared every year. In 2050, around the universe 135 millions will affect due to ageing peoples (2), (Bienias JL, et al.).
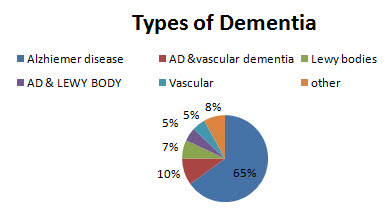
Types of Dementia
Dementia is broadly categorized into following types. There are Alzheimer’s disease, senile dementia, vascular Dementia, Dementia with levy bodies (DLB), Parkinson’s disease(PD), Frontotemporal dementia including Pick disease, Reversible causes of dementia (e.g., normal-pressure hydrocephalus, thyroid dysfunction, vitamin B12 deficiency, depression). The patient who has dementia they are usually characterized by following signs and symptoms:
A. Keeping track of things
B. Communication and language problem
C. Short term memory loss
D. Confusion. (3)
Sign of Dementia
The most common cause of dementia due to degenerative condition of the brain. It is employed gradual or progressive loss of memory and other cognitive functions usually in late life.
a) Memory loss: the dementia patient will forget all recently learned information. Normal information also gets forget, for example their names, relatives, phone numbers etc. They may be remember them later or does not remember longer.
b) Problems with language: The dementia people have trouble while speaking the right words or simple words to others. They are use unusual words, writing (hand writing) and difficult to understand.
c) Poor judgment: The AD people judge their self without believe anyone and their thinking no one has perfect and take the poor judgment.
d) Behavior changes: The unwanted changes will appear in the patient behavior; always they are felt in sad and depressed. When they are excited they are make some sounds and tear sometime.
e) Personality changes: The people’s personality changes from initial behavior on early stages of dementia. It may occur because of confusion, fearful ,dependent on a family member.(4)
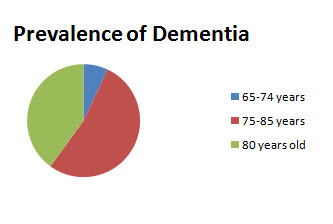
Prevalence of Dementia
The world wide prevalence of dementia is estimated to be 30 million people, with 4.6 million People affected annually. The number of people affected by dementia is predicted to be over 100 million by 2050. (5, 6) Onset of dementia can be as early as age 40 years, resulting in the arbitrary age classifications of early onset (ages 40 to 64 years) and late-onset (ages 65 years and older).(7,8) . The prevalence of Dementia increases exponentially with age, affects approximately 7% of individuals ages between 65 to 74 years, 53% of those ages 75 to 84, and 40% of persons ages 85 years and older.(9,33) Genetic causes is also a significant risk factor, although other factors may contribute.(7) AD is the fifth most common disease cause death. (10) AD may not cause death directly, but it predisposes patients to sepsis, trauma, pneumonia, choking and aspiration, and nutritional deficiencies mainly vitamin deficiencies. (11)
Diagnosis of Dementia
Dementia is first evaluated by a doctor who reviews the patient history and performs the physical examination. At present the only way to definitively diagnose AD is through direct examination of brain tissue at autopsy or biopsy. For patients who has dementia syndrome recommendations of Neurological examination include a neuroimaging study such as computed tomography (CT) or magnetic resonance imaging (MRI), as well as laboratory tests include serologic evaluation consists blood cell counts, serum electrolytes, liver function tests, a test of thyroid function, and a vitamin B-12 level.(12)AD is not the leading clear identity on the differential diagnosis, other neurologic tests also performed, such as spinal fluid analysis or electroencephalogram (EEG) can occasionally be justified to confirm the dementia syndrome. (13) A family member those who are felt in dementia or affected by memory complaints primary attention and care should be taken as soon as possible. Up to 50% of patients who felt in dementia are not given a diagnosis in the primary care setting, leading some to believe that screening tool may be helpful in aiding diagnosis and leading to earlier treatment. (14, 15)Unless the patient developed dementia prior to age 60 years and also had a parent that developed AD before age 60years .patient family history is also helpful diagnostic tool to screen the dementia. (16, 17)
Treatment of Dementia
The primary response of AD treatment is production of reduced cognitive difficulties and save the patient as long period. Although change the abnormal psychic and behavior in the severe condition. The current medication does not cure the disease it provides the temporary relief from AD. (18)
Cognitive symptoms treatment:
Alzheimer disease is treated with the use of cholinesterase inhibitors (Enhancement of cholinergic activity in patients with AD by inhibiting the hydrolysis of Ach through reversible inhibition of cholinesterase).Tacrine was the first drug used in treatment of AD. After the drug was usefulness due to its significant side effects like hepatotoxicity, diarrhoea, abdominal cramps, and polyuria. (19)
Cholinesterase inhibitors
Donepezil, rivastigmine, and galantamine are prescribed in mild to moderate AD, while donepezil is also indicated in severe disease. Memantine is indicated for moderate to severe AD. (20) When memantine is prescribed to cholinesterase inhibitor therapy in moderate to severe AD they produce better effect. In the combination therapy only one cholinesterase should be used (20, 21)
Donepezil: Donepezil is a predominant centrally acting ChE (cholinesterase) Inhibitor. It does not cause hepatotoxicity. It starts with the 5-mg dose and gradually increased into 10mg/ day. Donepezil is metabolized by Substrate (minor) of CYP2D6 and 3A4 under the process of glucuorinidation.
Rivastigmine: Rivastigmine is a ChE (cholinesterase) Inhibitor given in a dose 6-12mg/day for six months and has been show to improve cognitive functions in patients who have dementia, AD. Rivastigmine has central ChE inhibitory action.
Galantamine: Galantamine acts by dual mechanism such as inhibition of central ChE and as an agonist on central Ach nicotinic receptors. Galantamine is given in a dose 8-12mg/ twice a day for severe dementia and psychic patients. (20)
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
NMDA receptor inhibitors
Memantine: Excessive NMDA receptor activation can lead to excitatory toxicity and neuronal death. This suggests that memantine blocks pathological stimulation of NMDA receptors may protect against further tissue damage in patients with vascular dementia and possibly Alzheimer’s disease [63].memantine initiated with daily dose is 10 mg twice daily, achieved by a 3-weeks
Antiglutamatergic Therapy
Memantine is the only NMDA receptor antagonist used currently. Memantine blocks glutamatergic neurotransmission by antagonizing NMDA receptors. Glutamate is an excitatory neurotransmitter in the brain it involves in the improvement of learning and memory.(19) Memantine drug can initiated at 5 mg/day and gradually increased weekly by 5 mg/day to the effective dose of 10 mg twice daily.It may be given with or without food. (23
NON –COGNITIVE SYMPTOMS TREATMENT:
Most of the dementia patients are manifested by non-cognitive symptoms.they may be categorized as psychotic symptoms, disruptive behavior and depression. Effective treatment of this problem is important to deplete the stress condition and abnormal psychic problems
Anti-Depressents:
Depression is a common sign in patients with Alzheimer disease occurring in 50% of patients.the patient who receives the treatment with selective serotonin reuptake inhibitors (SSRIs) shows better therapauetic results in the drugs such as sertaline,citalopram,paroxetine and fluoxetine.(28) serotonin/ nor-epinephrine reuptake inhibitor such as venlafaxine may be alternative.(24) The drug trazodone prescribed to manage behavioural or depressive symptoms mainly it recommends for patient affected by insomnia with dementia.(25) “Mood stabilizer” anticonvulsants such as carbamazepine or valproic acid may be appropriate alternatives to elevate the mood condition sad into excitated state, but evidence is conflicting.(26
Antipsychotics:
Antipsychotics are widely used in the management of neuropsychiatric symptoms in AD. In this type management shows most of the atypical antipsychotics provide best action for particular neuropsychiatric symptoms. Food and Drug Administration (FDA) approval as an indication for the management of behavioral symptoms in AD. Based on the analysis, 17% to 18% of dementia patients show a treatment response to atypical antipsychotics (27). Neuropsychiatric drug initiated in Dementia is haloperidol (1-3 mg/day), Quetiapine (100-300mg/day), Risperidone (0.75-2mg/day), Ziprasidone (40-160mg/day), and Olanzapine (5-10mg/day). (19, 28, 29)
CONCLUSION
The Alzheimer disease is irreversible disease, widely the AD treated by Anti-psychotics and Anti-Depressant drugs. This category of drugs acts well versed and shown better results in the persons behavior and prevent the frequent mood changes. The AD people also doesn’t have the sense of their daily activities, All those things are erased from their brain (it denotes Exact unconsciousness).Apart from the drug treatment, the patient should be treated with good humanity by the people who are surrounding them, the family members must be take care in patient health, then only the patient will be survive with their needful.
REFERENCES
1. Alzheimer’s disease facts and figures. 2010. http://www.alz.org/documents custom/report alzfactsfigures 2010. Date of accession: 4 Feb 2013.
2. Lezak MD, Howieson DB, Luring DW. Neuropsychological Assessment. 4th ed. New York, NY: Oxford University Press; 2004.
3. Goedert M, Spillantini G. A century of Alzheimer’s disease. Science 2006; 314:777–781.
4.Benoit M, Arbus C, Blanchard F, et al. Professional consensus on the treatment of agitation, aggressive behavior, oppositional behavior and psychotic disturbances in dementia. J Nutr Health Aging 2006; 10:410–415.
5. Alzheimer’s disease International factsheet, The Prevalence of Dementia Worldwide,
(2008).
6 . A Wimo, B.Winblad, H. Aguero-Torres and E. V. Strauss, The magnitude of Dementia occurrence in the World, Alzheimer Disease and Associated Disorders, 17 (2) (2003), 63–67.
7. Alzheimer’s Association. http://www.alz.org/.
8. Nussbaum RL, Ellis CE. Alzheimer’s disease and Parkinson’s disease. N Engl J Med 2003; 348:1356–1364.
9. Hebert LE, Scherr PA, Bienias JL, et al. Alzheimer’s disease in the U.S. population: Prevalence estimates using the 2000 census. Arch Neurol 2003; 60:1119–1122.
10. Desai AK, Grossberg GT. Diagnosis and treatment of Alzheimer’s disease. Neurology 2005; 64 (Supplement 3):S34–S39.
11. Chandra V, Bharucha NE, Schoenberg BS. Conditions associated with Alzheimer’s disease at death: Case-control study. Neurology 1986; 36:209–211.
12. Mohs RC, Haroutunian V. Alzheimer’s disease: From earliest symptoms to end stage. In: Davis KL, Charney D, Coyle JT, Nemeroff C, eds. Neuro psychopharmacology: The Fifth Generation of Progress. New York: Lippincott Williams & Wilkins, 2002:1189–1198.
13. Boustani M, Peterson B, Hanson L, et al. screening for dementia in primary care: A summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2003; 138:927–937.
14. Knopman DS, DeKosky ST, and Cummings JL, et al. Practice parameter: Diagnosis of dementia (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001; 56:1143–1153.
15. Salmon E, Sadzot B, Maquet P, et al. Differential diagnosis of Alzheimer’s disease with PET. J Nucl Med 1994; 35:391–398.
16. Petersen RC, Smith GE, Ivnik RJ, et al. Apolipoprotein E status as a predictor of the development of Alzheimer’s disease in memory impaired individuals. JAMA 1995; 273:1274–1278.
17. Mayeux R, Saunders AM, Shea S, et al. Utility of the apolipoprotein E genotype in the diagnosis of Alzheimer’s disease. Alzheimer’s disease Centers Consortium on Apo lipoprotein E and Alzheimer’s disease. N Engl J Med 1998; 338:506–511.
18. Geldmacher DS, Frolich L, Doody RS, et al. Realistic expectations for treatment success in Alzheimer’s disease. J Nutr Health Aging 2006; 10:417–429.
19. Lleó A, Greenberg SM, Growdon JH. Current pharmacotherapy for Alzheimer’s disease. Annu Rev Med 2006; 57:513–533.
20. Lyketsos CG, Colenda CC, Beck C, et al. Position statement of the American Association for Geriatric Psychiatry regarding principles of care for patients with dementia resulting from Alzheimer’s disease. Am Geriatric Psychiatry 2006; 14:561–573.
21.McShane R, Areosa Sastre A,Minakaran N. Memantine for dementia. Cochrane Database Syst Rev 2006; 2:CD003154.
22. Lancelot E, Beal MF. Glutamate toxicity in chronic neurodegenerative disease. Prog Brain Res 1998; 116: 331-47.
23. “Memantine.” Geriatric Lexi-Drugs Online. http://www. Crlonline.com/crlonline
24. Lyketsos CG, Olin J. Depression in Alzheimer’s disease: Overview and treatment. Biol Psychiatry 2002; 52:243–252.
25. Rubin CD. The primary care of Alzheimer’s disease. Am J Med Sci 2006; 332:314–333.
26. Beier MT. Treatment strategies for the behavioral symptoms of Alzheimer’s
Disease: Focus on early pharmacologic intervention. Pharmacotherapy 2007; 27:399–411
27. Antipsychotic. Schneider LS, Tariot PN, Dagerman KS, et al. Effectiveness of atypical
drugs in patients with Alzheimer’s disease. N Engl J Med 2006; 355:1525–1538.
28. Benoit M, Arbus C, Blanchard F, et al. Professional consensus on the treatment of agitation, aggressive behaviors, oppositional behavior and psychotic disturbances in dementia. J Nutr Health Aging 2006; 10:410–415.
29. Grossberg GT, Desai AK. Management of Alzheimer’s disease. J Gerontol A Biol Sci Med Sci 2003; 58A:331–353.
30. Hebert LE, scherr PA, Bienias JL,et al. Alzheimer disease in the US population :prevalence estimates using the 2000 census. Arch neural 2003; 60:1119-1122.
31. Irudaya rajan s, mishra US sarma PS, India’s elderly: burden or challenge, new Delhi: sage publications and London: thousand oaks 1999.
32. Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, et al. (2013) The global prevalence of dementia: a systematic review and meta analysis. Alzheimer’s Dement 9: 63-75.
33. Chan KY, Wang W, Wu JJ, Liu L, Theodoratou E, et al. (2013) Epidemiology of Alzheimer’s disease and other forms of dementia in China, 1990-2010: a systematic review and analysis. Lancet 381: 2016-2023.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE