
About Authors:
Amardeep Sharma
Rathi Orthopaedic & research centre,
Ahmedabad, India
amardeep.sharma54@gmail.com
{ DOWNLOAD AS PDF }
ABSTRACT:-
The knowledge of breast cancer development and progression has grown in recent years and relatively development of novel therapeutic strategies, but for cancer mortalities in women breast cancer stands at 2nd position as cause.
In U.S. Approximately 39970 women & 450 men in the U.S. will be diagnosed from the disease in 2011.[1] Breast cancer is a hormone dependent disease.[3] Breast cancer occurs when breast epithelial cells grows in abnormal way. HER2/neu, ER, PR, BRCA1, BRCA2 are the well known influencing factors responsible for breast cancer initiation. The major issues that limit the currently available breast cancer treatment are high cost, poor availability and resistance to chemotherapeutic agents. To overcome this problem researchers are working on several novel approaches i.e. “Novel drug targets & Novel target therapies”.
Since from past few years, mammogram is playing a huge role for decreasing incidence rate in developed countries. Breast cancer is adversely affecting the “quality of life” of patients and its impact has been increasing on the Social capital, population structure and economic growth. Need for novel anti breast cancer agent and novel early diagnosis technique is necessary to combat one of the most serious crises facing Human development.
Reference Id: PHARMATUTOR-ART-1495
INTRODUCTION:
Breast cancer is a heterogeneous disease & since past 2 decades it has been estimated that breast cancer is a common malignancy in women of world. The data suggests that higher numbers of incidences are estimated in developed countries such as U.K., U.S., and CANADA but nowadays developing counties also suffers with the high numbers of breast cancer incidences. But past few years the incidences of breast cancer is continuously fallen in developed countries such as U.S., U.K. because of recent advancement in treatment & diagnosis approaches.
“The cells of breast become abnormally multiply without any control or order to form a cancerous tumor that is called Breast cancer”. Breast cancer starts from epithelial cell linings of the ducts (that work as a carrier of milk to the nipple) that called Ductal type of cancer. Similarly the other forms of breast cancer that starts in glands (that produce milk) that is called lobular cancer or in other parts of the breast. In case of later stage of breast cancer the cancerous tumor moves to other tissue or distance parts of the body.
If in case of breast cancer cells spreads (metastasize), cancerous cells most often appear in site of bones, liver, lungs, or brain. Tumors that starts at site and then spread to other areas of the body are called metastasize cancer and this type of breast cancer is incurable.]
INCIDENCES:-
“Breast cancer is a hormone-dependent disease. The age during menarche, 1st pregnancy, & fulltime menopause is the major factor responsible for the incidence of breast cancer in women.” [2].
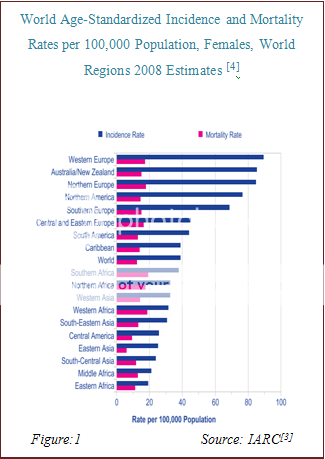
BY AGE: The breast cancer age standardized incidences of the worldin 2008(figure-1[3]) estimated by the ICD (International classification of disease) coding system set by the W.H.O. the data suggests that the incidences of breast cancer was high in Europe & U.S. countries than African & Asian counties. But from past few years the incidence rate are continuously coming dawn in developed countries [U.K. & U.S.]. It is estimated by American cancer society that the major factor behind reduced incidence rate is the regular mammograms.
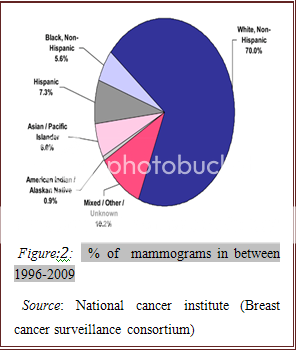
Mammograms impact on incidence
In developed countries routine mammogram is playing a key role for decreasing incidence rate. Figure:2 shows the data of women who taken mammogram in between 1975-2009.
PATHOLOGY: -
Breast cancer initiation and development has different types of pathways that depends on the various factors or receptor those responsible for the breast cancer initiation and progression.
Mutation in epithelial cell, HER-2, ER, PR, BRCA1 and BRCA2 are the main target or receptor for development of the breast cancer.
Pathology of hereditary breast cancer:
Various risk factors are responsible for breast cancer have been identified such as positive family history, early minarch,and a positive family history, late menopause, and nulliparity. The cause of breast cancer may include any one of this genetic, hormonal, lifestyle, dietary and environmental cause. A number of genes conferring high risk of breast cancer includes BRCA1 and BRCA2[4][5] P53 “Li-fraumeni syndrome” [6] & PTEN “Cowden syndrome”[7] have been identified where P53 and PTEN are associated with rare cancer syndrome. Almost it is clear that variants of many genes mediate the overall susceptibility of breast cancer. These genes are evidenced in literature such as RAD51, ATM, CHEK2, BRIP1, PALB2, and NBS1[8-12]conferring small to moderate risk of breast cancer.
It has been well known that BRCA1 and BRCA2 germline mutation resulting in breast cancer differ in different cases and the difference lies in morphology, molecular, and immunophenotype vary in age matched sporadic & familial breast cancer in non BRCA1 or 2 patient cases.[13-16]BRCA1 and BRCA2 perform regulation of cell cycle, DNA repair, transcriptional regulation & chromatin remodeling, regulation of RAD51 activities and DNA recombination respectively.
BRCA1 and BRCA2 functions loss leads to following activities such as non-conservative/error prone, potentially mutagenic and ultimately result into genomic instability contributing to the cancer predisposition.[17]
Clinical symptoms
v The general symptoms of breast cancer at early stage such as…
* Presence of lump or swelling as a mass.
* Arm pit (lymph node) swelling.
* Bloody or clear discharge from nipple.
* Nipple pain and retracted inverted nipple.
* Unusual breast pain
v Advanced stage of disease also some symptoms are mainly occurs such as…
* Bone painfulness (metastases in bone)
* Loss of appetite(Metastases in liver)
* weight loss(Metastases in liver)
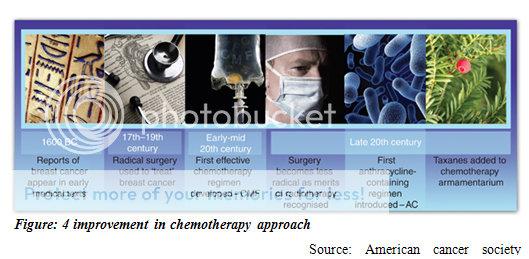
CURRENT TREATMENT APPROACHES & THEIR IMPACT:-
Cancer treatment can be local /systemic therapy:
* Local therapy: It includes Surgery and Radiation therapy:
Radiation therapy:
The process in which involves x-rays or other types of high energy radiations either for killing cancerous cells or to inhibit their growth.
The two types of radiation therapy are used in treatment of breast cancer.
1) External radiation therapy: - The process in which a machine that present from outside the body uses for sending radiation toward the cancerous cells and destroyed them.
2) Internal radiation therapy: - In this process involves the use of radioactive substance by wire, seeds, needle, (sealed) catheters for delivery it into or near by the cancerous cells/tumors.
The area of skin treated by radiation therapy may show some side effects after radiation therapy such as itchy, tenderness, redness, dry and breast may feel tight and heavy.
Surgery: Remove the cancer from the breast.
* Breast- conserving surgery: The removal of the cancer cells from breast but not the breast with the help of an operational procedure.
* Lumpectomy: A minor surgery for removal of the lump i.e. tumor as well as normal surrounding tissues.
* Partialmastectomy: It is a surgery process for the removal of cancerous breast part including surrounding normal tissue and suspected or required chest muscles epithelial lining under cancerous breast part may get removed.
* Totalmastectomy: As the name suggest thatin this process whole breast has removed that called total mastectomy and for biopsy of the under arm lymph node at the time of breast surgery that may be removed.
Side effectswith surgery i.e. pain, bleeding, swelling, and infection are possibilities seen after the surgery process
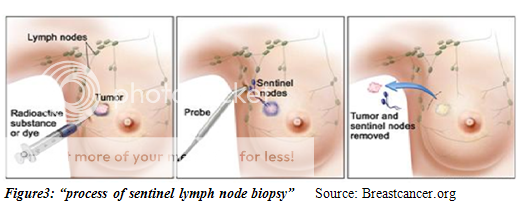
Biopsy of Sentinel lymph node
The removal of sentinel lymph node in between surgery for the purpose of Sentinellymph node biopsy.
In this method a specific radioactive substance is use to inject near the tumor and radioactive substance flows through the ducts of lymph to the lymph nodethan removed 1st lymph node who received the substance and examine either lymph node has cancerous cells or not.
Systemic therapy
Chemotherapy:
The main approach of chemotherapy in cancer treatment is to stopping cancer cells to divide or killing them by the use of drugs. Two types of chemo therapy methods are mostly used systemic chemotherapy and regional chemo therapy.
Adjuvant therapy are given after the completion of surgery process to reduce the chance of recurrence of breast cancer and neoadjuvant therapy are given before the surgery process to reduce or shrink the tumor size, surgery related decisions are made after neoadjuvant therapy.
Side effectswith chemotherapyi.e. diarrhea, fatigue, fertility issues, memory loss, menopause and menopausal symptoms, mouth and throat sores, vaginal dryness.
Targeted therapy: Targeted therapies are one of the important options to treat breast cancer with the help of drugs. The mechanism of targeted therapy is to identify the cancerous cells or tumors and directly attack on cancerous cells or tumors without causing any kind of harm to normal cells of the breast.
Nowadays tyrosine kinase inhibitors & monoclonal antibodies are mainly used as a targeted therapy for breast cancer.
A monoclonal antibody, Trastuzumab (Herceptin) is useful in treatment of HER-2 patient and trastuzumab blocks the effects of the HER2 protein. Tyrosine kinase inhibitors inhibit the tumors growth by blocking the signals that are needed for growth of tumors.
Hormone therapy: Hormones are one of the known causes of breast cancer. Hormone therapies are used against Estrogen+ve patient’s treatment. Tamoxifen is well established drug for treatment of Estrogen+ve since past two decade. Tamoxifen is the 1st discovered target therapy drug in the history of any cancer target therapy. But side effects such as hot flashes, discharge from vagina etc. limits the tamoxifen.
Limitation of currently available treatment approaches
Hormone therapy, Targeted therapy, surgery and radiation therapy are the currently available treatment approaches for breast cancer. Chemotherapeutic agents (trastuzumab, tamoxifen, bevasuzumab, lapatinib etc.) are plays a major role such as in hormone therapy, before or after surgery process, targeted therapy but side effects with chemotherapy, high cost of trastuzumab, bevasuzumab etc. limits the currently available treatment. High cost also limits the availabilities of these drugs.
The majority of patients who survive with metastatic breast cancer they initially respond to trastuzumab but after one year of treatment they shown resistance to trastuzumab.
Chemotherapy, radiation therapy, and surgery are causes some side effects that limit this approaches.
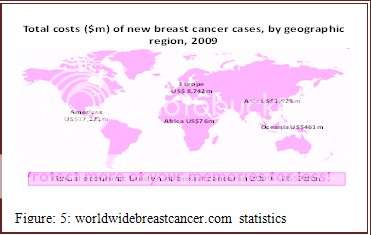
Cost and Availability: -
Breast cancer treatment high cost is mainly due to expensiveness of chemotherapeutic drugs and drugs that are used in target therapy such as trastuzumab, tamoxifen, bevasuzumab etc. The figure: 5 show that the whole world suffers with breast cancer high cost. Breast cancer treatment is expensive so it is not widely available so majority ofpatients do not have proper access to treatment approach which limits the therapy & promotes breast cancer burden globally.
Treatment-refractory patient:
Treatment refractory patients are also one of the major issues for current treatment approach that limits the effective therapy and chemotherapeutic agents those used in breast cancer treatment.Research had shown that currently most of patients are unresponsive to chemotherapy treatment.
Various types of mechanisms are known in that Cancer cells become resistant to chemotherapy. Here is one example for TRP. Expression of ABC transporters, including MDR1, leads to resistance through the active efflux of drugs, and each type of transporter is able to carry several different types of drugs, particularly anthracyclines and taxanes.[19]
Initiative treatment approaches
Novel drug targets:
Breast cancer called a heterogeneous disease and the early stage diagnosis of breast cancer is still a major problem associated with early stage cure or treatment.
Nowadays, the researchers are mainly focused on novel drug targets approach for directly attack on the breast cancer specific target and terminate there action. Several of targets are found and currently in evaluation.
Table: 1: - Novel drug targets in clinical trial
|
Agents |
Application |
Clinical Phase of development |
Targets |
Ref. |
|||
|
Lapatinib and capecitabine versus capecitabine |
Advanced breast cancer |
iii |
EGFR, HER+ |
20,21 |
|||
|
Lapatinib and paclitaxel |
Inflammantory, neoadjuvent |
ii |
EGFR,HER+ |
22 |
|||
|
Ad5CMV-p53 and docetuxel/doxorubicin |
Primary BC, neoadjuvent |
ii |
p53 |
23 |
|||
|
Tipifarnib and gemcitabine |
|
Metastatic BC |
ii |
Ras, Farnesyl transferase |
24 |
||
|
Tipifarnib and letrozole |
|
Advanced BC |
ii |
Ras, Farnesyl transferase |
25 |
||
|
Lanafarnib and anastrozole |
|
Metastatic BC |
ii |
Ras, Farnesyl transferase |
24 |
||
|
Bortezomib |
|
Metastatic BC |
ii |
26S Proteasome |
26 |
||
|
Bortezomib |
|
Metastatic BC |
ii |
26S Proteasome |
27 |
||
|
Agents |
|
Application |
Clinical Phase of development |
Targets |
Ref. |
||
|
Bortezomib |
|
Metastatic BC |
i |
26S Proteasome |
28 |
||
|
Bevacizumab |
Metastatic BC |
i/ii |
VEGF |
29 |
|||
|
Bevacizumab |
Metastatic BC |
ii |
VEGF |
30 |
|||
|
Cetuximab and paclitaxel |
Advanced BC |
iii |
EGFR |
31 |
|||
|
Erlotinib |
Primary BC,Neoadjuvent |
i |
EGFR |
32 |
|||
|
Evorolimus(RAD-001) |
Primory BC, Neoadjuvent |
iii |
mTORi |
38 |
|||
|
Evorolimus(RAD-001) |
Metastatic BC, Bone metastatic |
ii |
mTORi |
38 |
|||
|
Pertuzumab |
|
i |
mAb,HER2 |
33 |
|||
|
E1A |
|
i |
Transcriptional inhibitor |
33 |
|||
|
AutoVac ® |
|
ii |
DNA Vaccine |
33 |
|||
Novel target therapies: -
Selection of agents, timing of initiation and discontinuation, and incorporation of novel therapies remain both a science and an art. For many patients, sequential use of different therapies can translate into years of prolonged survival with preserved quality of life. Several novel targets are currently in clinical trial.
Nanotechnology: Clinical trial investigating efficacy of target based drug delivery system using nano-carriersapproach leading to anti tumor activity.
Table2:- Drug therapy [34]
|
Drug therapy |
Drug |
In development |
Cancer type |
|
Polymeric- Nanoparticles (50–200) |
Doxorubicin, Paclitaxel platinum based drugs, Docetaxel |
Several products are in |
metastatic breast cancer |
Gene therapy: recent vast knowledge of tumor suppressors genes and proto-onco genes in genesis of malignancy leads to development of various gene therapy tactits. Some are based on ablation or restoration of such vitally involved genes and some are based on immune system modulation which can activate the mechanism of anticancer drug defense targeting at drug resistance genes to combat drug resistance. [35]
Oncogenes Inactivation: - Antisense strategies to oncogenic proteins is widely undergoing via clinical trials. An approach is to inhibit the transcription of oncogene by E1A (adenoviral gene) that too hinders the transcription of erbB2 is useful in over expressing oncogenic protein cancer.[35]
Augmentation of tumor suppresser genes: - Over several number of tumors suppressor gene mutation associated with variety of neoplasia have been identified, and the stratigies is to use the vector such as adenoviral vector for delivery p53 and genetic repair strategy is another effective approach. [36]
Cell- target suicide: - An approach of creating an artificial difference between neoplastic & normal tissue via prodrug conversion into toxic metabolite by genetically engineering tumor cells.[37]
Chemo protection, ectopic cytokine expression, virus mediated oncolysis immune enhancement, immune modulation are some of the other important ongoing approaches to combat the burden of breast cancer.[36], anti HER-2 target therapy.
Discussion
Critical assessment on novel target therapy
Overexpressions of HER-2 /neu protein have been evidenced in 20-30% of metastatic breast cancer and numerous numbers of patients are affected with HER-2 ovrexpression.
HER-2(neu) is a potential novel target for treatment of metastatic breast cancer. Till now metastatic breast cancer is a incurable disease so a reliable & therapeutically effective drug (single/with combination) or novel target is required for treatment or improvement in “disease free survival” of the patient but the major issue associated with anti HER-2 target therapy is most reliable or efficient ASSAY is not available for detection of HER-2 status (prognosis/response).
Some of the pre-clinical studies data suggests that some molecular targeted agents have given low response whenever they evaluate in clinical trial.[38]
Various challenging issues associated with Novel HER-2 target therapy such as side effects, high cost and resistance to chemotherapeutical agents, “incurability of metastatic breast cancer”.
Conclusion: -
To successfully overcome with breast cancer, various novel target therapies & new diagnosis approaches are currently in clinical evaluation. Mammography plays a major role in reduction of incidences. Metastatic breast cancer still incurable but HER-2 is a potential novel target & will be useful for improve “quality of life” & survival of patients.
References:
1. Osteen, R. Breast Cancer. In: Lenhard RE, Osteen RT, Gansler R, eds. Clinical Oncology. Atlanta, GA: American Cancer Society; 2001:251–268.
2. Dennis L. Kasper, Eugene Braunwald, Anthony S. fauci et al. Harrisson’s Principle of Internal Medicine. McGraw Hill, Medical Publishing Division. 16Th Edition, 516-517.
3. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM, GLOBOCAN 2008 v1.2, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10 [Internet] Lyon, France: International Agency for Research on Cancer; 2010. Available from: https://globocan.iarc.fr
4. Miki Y, Swensen J, Shattuck-Eidens D, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994;266: 66–71. |
5. Wooster R, Bignell G, Lancaster J, et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995;378:789–792
6. Easton D, Ford D, Peto J. Inherited susceptibility to breast cancer. Cancer Surv 1993; 18, 95–113.
7. Lynch ED, Ostermeyer EA, Lee MK, et al. Inherited mutations in PTEN that are associated with breast cancer, cowden disease, and juvenile polyposis.Am J Hum Genet 1997; 61, 1254–1260.
8. McKinnon PJ. ATM and ataxia telangiectasia. EMBO Rep 2004;5:772–776.
9. Nevanlinna H, Bartek J. The CHEK2 gene and inherited breast cancer susceptibility. Oncogene 2006;25:5912–5919.
10. Rahman N, Scott RH. Cancer genes associated with phenotypes in monoallelic and biallelic mutation carriers: new lessons from old players. Hum Mol Genet 2007;16(Spec No. 1):R60–R66.
11. Rahman N, Seal S, Thompson D, et al. PALB2, which encodes a BRCA2-interacting protein, is a breast cancer susceptibility gene. Nat Genet2007;39:165–167.
12. Stratton MR, Rahman N. The emerging landscape of breast cancer susceptibility. Nat Genet 2008;40:17–22.
13. Wooster R, Bignell G, Lancaster J, et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995;378:789–792.
14. Wooster R, Neuhausen SL, Mangion J, et al. Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science1994;265:2088–2090.
15. Armes JE, Egan AJ, Southey MC, et al. The histologic phenotypes of breast carcinoma occurring before age 40 years in women with and without BRCA1 or BRCA2 germline mutations: a population-based study. Cancer1998;83:2335–2345.
16. Armes JE, Trute L, White D, et al. Distinct molecular pathogeneses of early-onset breast cancers in BRCA1 and BRCA2 mutation carriers: a population-based study. Cancer Res 1999;59:2011–2017.
17. Venkitaraman AR. Cancer susceptibility and the functions of BRCA1 and BRCA2. Cell 2002;108:171–182.
18. worldwidebreastcancer.com/risks/breast-cancer-world-statistics/
19. Szakacs G, Paterson JK, Ludwig JA, Booth-Genthe C, Gottesman MM. Targeting multidrug resistance in cancer. Nat Rev Drug Discov. 2006;5:219-234.
20. Reid A, Vidal L, shaw H, de Bono: Dual inhibition of ErbB1(EGFR/HER1) and ErbB2(HER2/neu), Eurj cancer 2007, 43, 481-489.
21. Geyer CE, Forster J , Lind quist D, et al. Lapatinib plus capecita- bine for HER-2 positive advanced breast cancer. N Engl J Med 2006, 355, 2733-2743.
22. Cristofanilli M, boussen H, Baselga J, et al. A Phase ii combination study of lapatinib and paclitaxel as a neoadjuvent therapy in patients with newly diagnosed inflammantory breast cancer (IBC) san antonio Breast cancer symposium 2006, Abstract Nr.1, General session.
23. Cristofanilli M, Krisnamurthy S, Guerr L, A nonreplicating adeno-viral vector that contains the wild- type p53 transgenes combined with chemotherapy for primary breast cancer: Safety, efficacy, and biologic activity of a novel gene therapy approach. Cancer 2006, 107, 935-944.
24. Appels Nm, Beijnen JH; Schellens JH. Development of farnesyl transferase inhibitor: a review. Oncologist 2005, 10, 565-578.
25. Gligorav J, Azria D, Namer M et al: Novel therapeutic strategies combining antihormonal & biological targeted therapies in breast cancer: Focus o clinical trials and perspectives. Crit Rev. Oncol Hematol 2007, 64, 115-128.
26. Yang CH, Gonzalez-Angulo AM, Reuben JM, et al: Bortezomid(velcade) in metastatic breast cancer: pharmacodynamics, biological effects, and prediction of clinical benefits. Ann oncol 2006, 17; 813-817.
27. Engel RH, Brown JA, Van Roenn JH et al; A Phase ii study of single agent bortezomib in patients with metastatic breast cancer: a single institution experience. Cancer invest 2007, 25, 733-737.
28. Cardoso F, Durbecq V, Laes JF, et al; Bortezomib (PS-341, Velcade) increase the efficacy of Trastuzumab(Herceptin) in HER-2 positive breast cancer cells in a synergistic manner. Mol. Cancer ther. 2006, 5; 3042-3051.
29. Cobleigh MA, Langmuir VK, Sledge GW et al: A Phase i/ii dose- escalation trial of bevacizumab in previously treated metastatic breast cancer. Semin oncol 2003, 30,: 117-124.
30. Sledge G, Miller K, Novotny W, et al;: A Phase ii trial of single – agent rhumab VEGF (recombinant humanized monoclonal antibody to vascular endothelial cell growth factor) in patients with relapsed metastatic breast cancer (Abstract 5c) proc Am soc clin oncol 2000, 19:3a.
31. Madi S, D’Andrea G, Norton L, et al. APhase I study of cetuzumab/ pacclitaxel in patients with advanced- stage breast cancer. Clin breast cancer 2006, 7,: 270-277.
32. Guix M, Granja Nde, Meszoely et al. Short preoperative opration with erlotinib inhibit tumor cell proliferation in hormone receptor positive breast cancer. J Clin oncol, 2008, 26, 897-900.
33. Rita Nahta, Dihua Yu, Mien- Chie Hung et al; Mechanism of disease understanding resistance to HER-2 targeted therapy in human breast cancer. Nature practice oncology, may 2006, 3(No.5), 275.
34. Dan Peer, Jeffrey M. KarP, SeungPyo Hong, et al. Nanocarriers as an emerging platform for cancer therapy.nature nanotechnology. DECEMBER 2007, 2, 755.
35. Osborne C., Wilson P., tripathy D. oncogenes and tumor suppressor genes in breast cancer. Potential diagnostic and therapeutic applications. The oncologist. 2004,9, 361-377.
36. Ganesh N Sharma, Rahul dave, Jyotsana sanadya et al. Various types and management of breast cancer: An overview, J. Adv. Pharm. Tech. Res. Apr-jun,2010 1(2), 119-121.
37. Jin-Hui W., Xin- Yuan L. targeting strategies in cancer gene therapy. ACTA Biochimica and biophysica sinica. 2003; 35, 311-316.
38. Claus M Schlotter,Ulf Vogt, Heike Allgayer and Burkhard Brandt. Molecular targeted therapies for breast cancer treatment. BioMed Central Ltd., Breast Cancer Research 2008, 10:211(doi:10.1186/bcr2112).
|
PharmaTutor (ISSN: 2347 - 7881) Volume 1, Issue 1 Received On: 08/10/2013; Accepted On: 02/11/2013; Published On: 25/11/2013 How to cite this article: Sharma A, Breast Cancer: An Overview, PharmaTutor, 2013, 1(1), 29-38 |
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE








