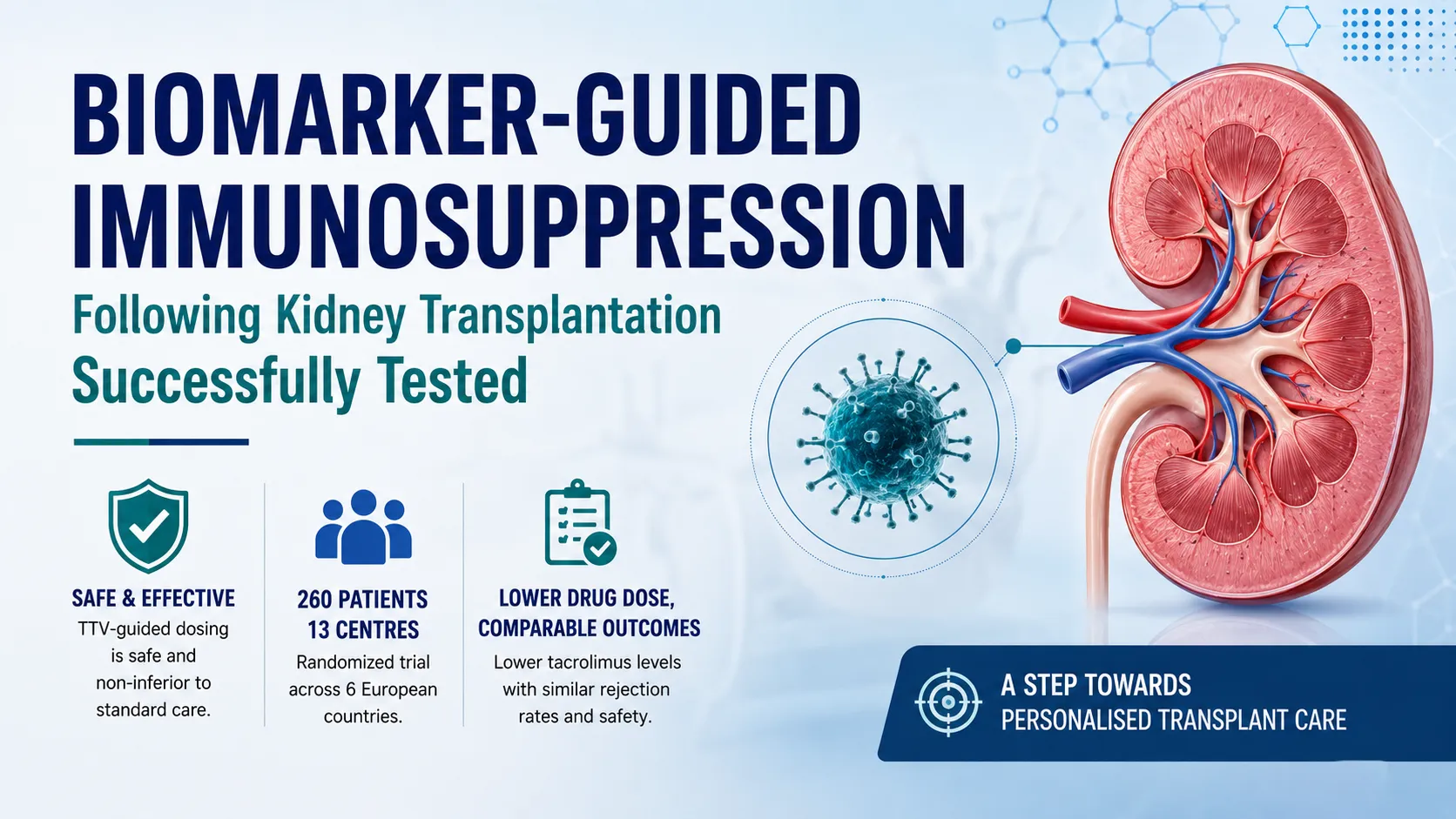
A groundbreaking European clinical trial has shown that using a common, harmless virus as a biomarker to guide immunosuppressive treatment after kidney transplantation is both safe and effective, paving the way for more personalized transplant care.
Researchers from the Medical University of Vienna, who coordinated the multinational TTVguideIT study, reported that monitoring levels of Torque-Teno Virus (TTV) can help tailor immunosuppressive therapy to individual patients without increasing the risk of organ rejection or other serious complications.
Kidney transplant recipients require lifelong immunosuppressive medications to prevent their immune systems from attacking the transplanted organ. However, finding the right balance is challenging. Excessive immunosuppression increases the risk of infections, while insufficient suppression can lead to organ rejection and graft failure.
Traditionally, physicians adjust treatment based on blood concentrations of immunosuppressive drugs such as tacrolimus. While useful, these measurements do not always reflect the actual state of a patient’s immune system.
The TTVguideIT study explored whether levels of Torque-Teno Virus, a virus commonly present in healthy individuals without causing disease,
could serve as a more reliable indicator of immune activity. Lower TTV levels may suggest stronger immune activity, while higher levels can indicate greater immune suppression.
“Our goal was to move beyond fixed drug targets and better align treatment with each patient's actual immunological status,” said Gregor Bond, project coordinator and nephrology specialist at the Medical University of Vienna.
The Phase II randomized controlled trial enrolled 260 stable adult kidney transplant recipients considered to have low immunological and infectious disease risk. Conducted across 13 academic centers in Austria, Germany, France, the Czech Republic, the Netherlands, and Spain, the study compared TTV-guided tacrolimus dosing with conventional treatment beginning four months after transplantation.
Researchers evaluated a composite primary endpoint that included infections, organ rejection, graft loss, and death. The endpoint occurred in 35% of patients receiving TTV-guided therapy compared with 38% of patients receiving standard care, demonstrating that the biomarker-guided approach was not inferior to conventional treatment.
Importantly, patients in the TTV-guided group maintained lower tacrolimus blood levels and required lower daily doses of the drug. Although the study did not show a statistically significant reduction in infections, the findings indicate that immunosuppression can potentially be reduced safely in selected low-risk patients.
The study also found comparable rejection rates between the two groups based on protocol biopsies performed one year after transplantation.
Experts believe the findings represent a significant advance in personalized transplant medicine. TTV testing is already approved for clinical use, is relatively inexpensive, easy to perform, and can be standardized across laboratories, making it a practical option for wider adoption.
The research formed the centerpiece of the Horizon 2020-funded TTVguideTX project, which received more than €6 million in European Union funding over five and a half years. The initiative involved 20 partners from 10 European countries, including transplant centers, virology experts, statisticians, ethics specialists, and industry collaborators.
Beyond its scientific significance, the project marked an important milestone for clinical research in Austria. It became the country’s largest investigator-driven randomized clinical trial and the first to bring together all four Austrian transplant centers in a single randomized study.
Researchers caution that the current findings apply primarily to stable, low-risk adult kidney transplant recipients during the first year after transplantation. Additional studies are needed to determine whether the approach can benefit higher-risk patients, individuals further removed from transplantation, or recipients of other transplanted organs.
To answer these questions, a follow-up multicenter study is already underway in France. Investigators hope to determine whether TTV-guided immunosuppression can provide further clinical benefits during the later years following transplantation.
If confirmed in future trials, biomarker-guided treatment could help physicians move closer to truly individualized transplant care, improving long-term outcomes while minimizing unnecessary exposure to immunosuppressive drugs.