
ABOUT AUTHORS
Navneet Kaur1, Latika Khosla2
1Department of Biotechnology, CT Institute of Pharmaceutical Sciences, Shahpur, Jalandhar-144001, Punjab.
2Department of Biotechnology, Kanya Maha Vidyalaya, Jalandhar-144004, Punjab
ABSTRACT
Diabetic nephropathy (DN) is defined as a progressive pathological condition of the kidney caused by angiopathy of glomerular capillaries. The angiopathy of these capillaries is characterized by a progressive loss of glomerular filtration surface areas and capillary volume. DN is the leading cause of end-stage renal disease, and a major contributing factor to morbidity and mortality of diabetic patients throughout the world.
INTRODUCTION
Diabetic nephropathy (DN) is one of the most common and serious long-term complications in diabetic patients, affecting about 40% of these patients (Ritz et al.1999; Gumzler et al.2013). Diabetic nephropathy is the leading cause of end stage renal failure (ESRF) worldwide, representing over 50% of patients on renal replacement therapy in some parts of the world. The condition is common in people with type 1 and type 2 diabetes, although the incidence appears to be declining, especially in type 1 diabetes. More than 1 in 3 people with type 2 diabetes have impaired kidney function (Manash et, al.2017). As the incidence of diabetes is increasing worldwide, diabetic nephropathy has become the main cause of chronic kidney disease in patients who require renal replacement therapy in the Western world, also known as Kimmelstiel-Wilson syndrome( Douglas et,al.2013).It is characterized by glomerular hypertrophy, thickness of basement, tubular and glomerular membranes and accumulation of extracellular matrix in these membranes that finally cause tubulointerstitial and glomerular fibrosis and sclerosis(Alsaad et al.2007)
There are five stages of diabetic nephropathy :( Themis et al.2009)
Stage I: The size of the kidneys is increased by approximately 20% and renal plasma flow is increased by 10%-15%, while albuminuria and blood pressure remain within the normal range
Stage II: The quiet stage. This stage starts approximately two years after the onset of the disease and is characterized by kidney damage with basement membrane thickening and mesangial proliferation.
Stage III:. It usually occurs five to ten years after the onset of the disease. Blood pressure may be increased or normal. Approximately 40% of patients reach this stage3-4.
Stage IV: Proteinuria develops (albumin > 300 mg/dU), GFR decreases below 60 ml/min/1.73 m2, and blood pressure increases above normal values
Stage V: Approximately 50% of the patients with TKF require kidney replacement therapy (peritoneal dialysis, hemodialysis, kidney transplantation)
Risk Factors for Diabetic Nephropathy (Harrison et al.1989; Ramachandran.1993)
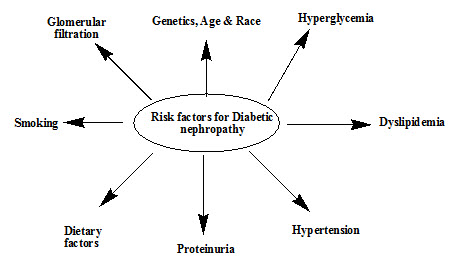
Figure No.1: Risk factors for Diabetic nephropathy
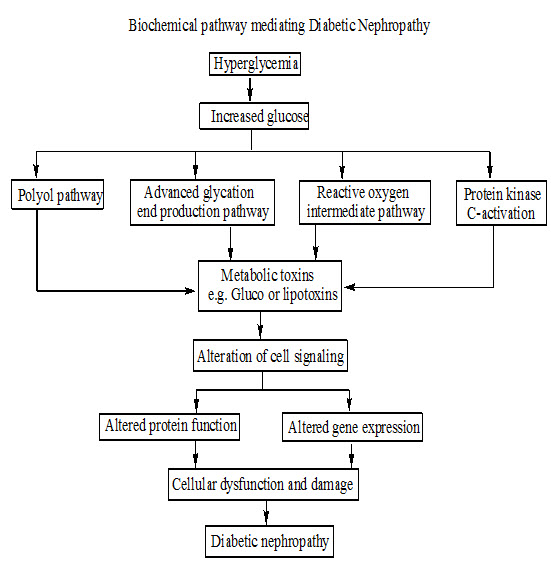
Figure No.2 : Pathogenesis of Diabetic nephropathy
Management of Diabetic nephropathy
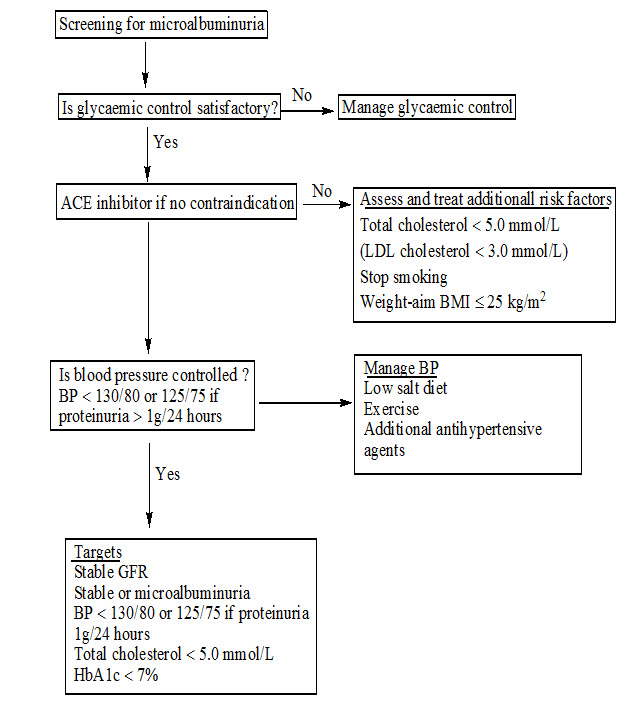
Figure No. 3 : Management of Diabetic nephropathy
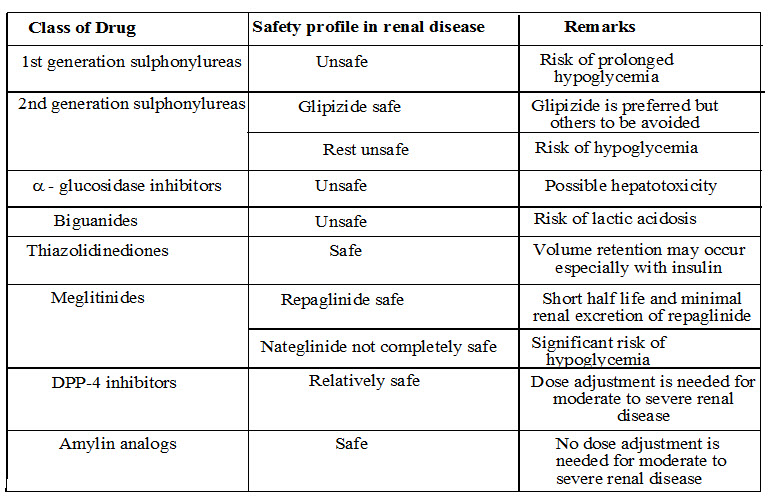
Hypoglycemic agents in diabetic nephropathy
Method of Evaluation of Therapeutic Agents for Nephropathy (Laspina et al, 2008; Malarkodi et al. 2003;Ohtake et al. 2002;Gvozdenko et al, 2004; Corley et al, 2008;)
Animal models for Nephropathy
The animal models for nephropathy which are common to human nephropathy and have been delineated by targeting proteinuria, glomerulosclerosis, glomerulonephritis, glomerular hypertrophy, tubule interstitial nephritis, tubular necrosis and reduced GFR.
• Diabetes-induced nephropathy
• Ciclosporin A-induced nephropathy
• Anthracycline-induced nephropathy
• Electrolyte nephropathy
• Ethylene glycol-induced nephropathy
• Aminoglycoside-induced nephropathy
• Cadmium-induced nephropathy
• Carbon tetrachloride-induced nephropathy
• Germanium dioxide-induced nephropathy
• Mercury chloride-induced nephropathy
• Cisplatin-induced nephropathy
• Vomitoxin-induced nephropathy
• Maleic acid-induced nephropathy
• Contrast-induced nephropathy
Different parameters used to evaluate Diabetic nephropathy
Biochemical parameters
• Blood glucose level
• Serum creatinine level
• Blood nitrogen urea
• Triglyceride
• Cholesterol
Physiological parameter
• Body weight
Antioxidant (TBARS)
CONCLUSION
In the last few decades developing weight of diabetes and its related DN, the phases of renal association in diabetes, and the treatment procedures to forestall or interfere with the movement of diabetic nephropathy and examination into treatments to treat DN is extending, for example, administrations and Risk factors.
REFERENCES
• Harrison, Kharbanda, Cunningham, McLellan, Hayes. Distribution of glutathione S-transferase isoenzymes in human kidney: basis for possible markers of renal injury. J Clin Pathol. 1989; 42(6): 624-8.
• B. Manash, L. Mangala, A. Sahabudin, C. Liakat, K. Saurabh. Small molecule inhibiting nuclear factor-kB Ameliorates oxidative stress and supresses renal inflammation in early stage of alloxan induced diabetic nephropathy in rats. Journal of Basic & Clinical Pharmacology. 2017;120(5):442-449.
• D. Gunzler , AJ. Bleyer , RL. Thomas , GB. Russell , A.Sattar . Diabetic nephropathy in a sibling and albuminuria predict early GFR decline: a prospective cohort study. Journal of Bio Med Nephrology. 2013;14(12):124-126.
• E. Ritz, S. Orth. Nephropathy in patients with type 2 diabetes mellitus. Journal of the National Medical Association. 1999;341(15):1127-33.
• G. Douglas, B. Anthony, T. Robort. Diabetic nephropathy in a sibling and albuminuria predict early GFR decline: a prospective cohort study. Journal of Bio Med central Nephrology. 2013;14(10):124-150.
• K. Alsaad, A. Herzenberg. Distinguishing diabetic nephropathy from other causes of glomerulosclerosis: an update. Journal of Clinical Pathology. 2007; 60(1): 18–26.
• Ramachandran, Viswanathan, Mohan. Epidemiology of NIDDM in Indians. J Assoc Phy India. 1993; 65(1): 1-4.
• Z. Themis, G. Fernado, B. Amely. Diabetology and Metabolic Syndrome. Bio Med Central. 2009;12(8):1-10.
• Laspina, Tripathi, Gatto, Bruch, Maier, Kittur. An interleukin-6-neutralizing antibody prevents cyclosporine-induced nephrotoxicity in mice. J Surg Res. 2008; 148: 121-125.
• Malarkodi & Varalakshmi. Lipoic acid as a rescue agent for adriamycin-induced hyperlipidemic nephropathy in rats. Nutr Res. 2003; 23: 539-548.
• Ohtake, Kimura, Takemura, Hishida. Effects of dietary lipids on daunomycin-induced nephropathy in mice: comparison between cod liver oil and soybean oil. Lipids. 2002; 37: 359-366.
• Gvozdenko, Novgorodtseva, Vostrikova, Kapitonova. Simulation of electrolyte nephropathy in rats. Bull Exp Biol Med. 2004; 138: 238-240.
• Corley, Wilson, Hard. Dosimetry considerations in the enhanced sensitivity of male wistar rats to chronic ethylene glycol-induced nephrotoxicity. Toxicol Appl Pharmacol. 2008; 228: 165-178.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
FIND OUT MORE ARTICLES AT OUR DATABASE








