About Authors:
M.sandhya sree*, Sowmya**
*Assistant Professor ,
Department of pharmacology,
BA&KR pharmacy college,
JNTUK, Andhra Pradesh.
**MBBS,GMC,
Guntur, Andhra Pradesh.
Abstract:
The study was conducted in two villages of Guntur district (Andra Pradesh) to determine the nature and extent of health problems of rural women. The data were collected from one hundred randomly selected rural ladies by interviewing them with the help of an interview schedule developed for the purpose.
The identified health problems were classified. The findings of the study indicated the prevalence of a number of health problems among rural women and a need was felt for their education on health aspects. A sizeable number of them were found to have suffered from bronchitis, coryza, indigestion, constipation, diarrhea , conjunctivitis, dandruff, tartar deposits on teeth, skin diseases, gynecological diseases and some other diseases like rheumatism, arthritis, etc.
The existence of a government hospital in village had no association of significant level with the health problems of rural women. Majority of the respondents perceived the treatment given in government hospital to be not effective and several other constraints in availing of the treatment facilities.
[adsense:336x280:8701650588]
Reference Id: PHARMATUTOR-ART-1232
Health is an asset to man and to his community and has come to be regarded as a prerequisite to socio-economic development. The active role of women in the development of agriculture, animal husbandry, village cottage industries and several other facets of rural life besides the home and family is well established and is a known fact. It would be not proper to think of economic development in rural areas, without active involvement and participation of the women folk in the development programmes. In the development programmes, it would also be unwise to expect active participation and involvement of individuals who are not fit or unhealthy. Often women because of their household responsibilities and ignorance of health and hygiene practices tend to neglect their illness till their health problems get aggravated and they become too sick to move around and attend to their normal household chores. All the more, they are dependent on others in the family to get
They needed medical attention. According to an estimate, fifty per cent of rural women in the country are daily wage earners and they do not have time to go to hospital without losing their wages. As a consequence of this vicious circle, inadequate medical facilities in rural areas and poor resources to obtain treatment from private medical practitioners, women in villages is often become a victim of a number of health problems.
Two-third of the population in the country consists of women of child bearing age and children under the age of fifteen years. Since, they constitute a particularly vulnerable group; they suffer most severely from consequences of socio-economic development. The existing health services being provided through a network of government hospitals, dispensaries, and primary health centers’ not reach or remain underutilized by women, especially, in rural areas. Otherwise also, the health care provided to rural areas is glaringly disproportionate to the needs and abnormally low as compared to urban areas. Under these circumstances, it was considered worthwhile to take a stock of the health status of rural women. With this background, the present study was undertaken to determine the nature and extent of health problems of rural women and constraints encountered by them in availing of the treatment facilities being provided by the government hospitals.
METHODOLOGY
The study was conducted in purposively selected Guntur district (Andrapradesh). Two villages, namely Gorantla and N ambur selected randomly, one of these had a government hospital and the other had no government hospital or a dispensary. About one hundred households (50 households from each of the two villages) were selected randomly. The female head of the family irrespective of its being a joint or nuclear family constituted the respondents of the study.
Health problem referred to any type of disease or sickness which may affect the health or general well being of the rural women. The nature of health problem referred to its being contagious or of non-contagious type.
The extent of health problem referred to the degree of prevalence of a disease or sickness at a given period of time in an area.
For studying the health problems, the data were collected by interviewing the respondents with the help of an interview schedule containing structured questions. The instrument of observation was prepared by vigorously going through the standard procedures prescribed for the purpose including the testing of reliability and validity. The diseases which had actually affected them during one year preceding the date of data collection or at the time of observation were identified. The records available with the respondents in the form of OPD tickets, prescriptions, etc., were also examined to determine their health problems. The constraints in obtaining medical aid from government hospitals were studied with the help of a close-end question developed for the purpose.
[adsense:468x15:2204050025]
RESULTS AND DISCUSSION
The health problems of rural women brought out by the study are shown in Table 1. A perusal of the table will indicate that more or less half of rural women had suffered from bronchitis (53 per cent) and coryza (48 per cent). Those suffering from asthma were 16 per cent. Majority of the people who were engaged in farming suffered from respiratory diseases'. Obviously then, prevention and control of respiratory diseases require special attention of the health department and specialized programmes need to be initiated.
The diseases of digestive system found among them were indigestion (29 per cent), constipation (23 per cent), diarrhea (17 per cent) and enteric fever (9 per cent). The diseases of gastro-intestinal tract mostly composed of diarrhea and dysentery were maximum in rural society2. Lack of sanitation coupled with polluted water caused such diseases3. The widespread habit of defecating in fields in the vicinity of villages or in stream beds or on pathways so that water or flies transfers the amoeba or bacilli to the human mouth could be the main cause of these ailments.
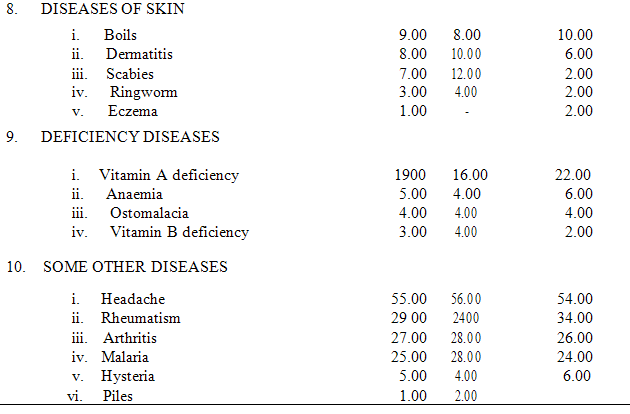
TABLE 1
DISEASES PREVALENT AMONG RURAL WOMEN
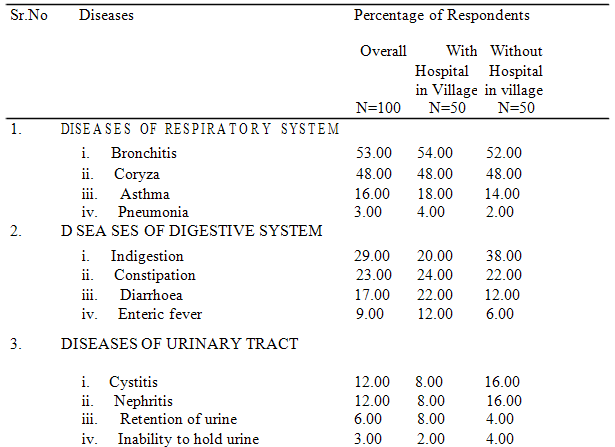
The study indicated that 12 per cent of rural women had suffered from cystitis and nephritis. The diseases like retention of urine and inability to hold urine were also reported though in a lesser proportion. The factors responsible for causing these diseases could be varied and many. Poor personal hygiene could be one of the predisposing factors for some of these diseases. Vaginal examination in such disease conditions is often refused by village people. As a consequence, problems are encountered in diagnosis and treatment. Moreover, the availability of diagnostic and treatment facilities for such type of ailments in villages is a remote possibility.
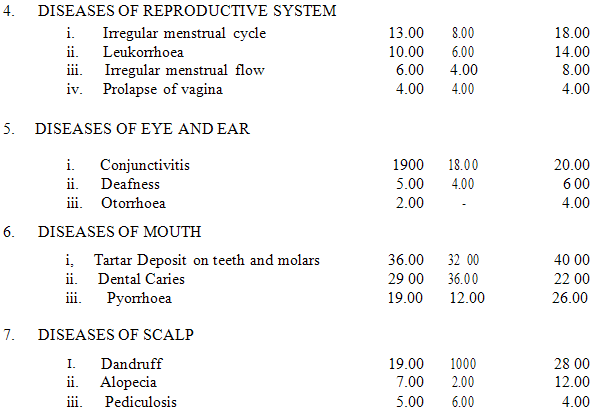
The diseases of reproductive system prevalent among rural women were irregular menstrual cycle (13 per cent), leucorrhoea (10 per cent), and irregular menstrual flow (6 per cent) and prolapse of vagina (4 per cent). These diseases could be due to faulty dietary pattern or . Due to hormonal disturbances . Irregular menstrual cycle or flow could be due to anemia resulting from malnutrition or dysfunction of ovaries besides several other causes. General debility could be a predisposing factor for leucorrhoea. Prolapse of vagina might be due to repeated pregnancies, child delivering by untrained women or nurses and carrying of heavy loads when pregnant, lack of rest, etc. For want of proper guidance, non-availability of a lady doctor for consultation and treatment in villages, and lack of resources for getting treatment from specialists located in towns, the women suffering from reproductive diseases either remain untreated or get delayed medical attention. In most of the cases indigenous treatment suggested by elderly women is often tried.
The study further revealed that 19 per cent of rural women suffered from conjunctivitis. Lack of hygiene and unhealthy environment cause diseases of eye like conjunctivitis4. The untreated recurrent infections may result in total blindness in about (1 per cent) and defective vision in (4 per cent) cases5. Deafness (5 percent) and otorrhoea (2 per cent) result from injuries to ears which remain untreated in early stages . These disease conditions need specialized treatment which is often beyond the reach of the rural people. For treatment of such ailments indigenous practices, such as, stuffing the ears with chalk powder and animal urine are tried which further aggravates the condition leading to incurable proportions.
A sizeable number of rural women had tartar deposit on teeth and molars (36 per cent), dental caries (29 per cent), and pyorrhea (19 per cent). The prevalence of dental fluorosis is directly proportional to fluoride concentration of drinking water and dental caries is associated with fluorosis4. Lack of oral Hygiene often results in tartar deposit on teeth and molars.
The diseases of scalp afflicting the rural women were observed to be dandruff (19 per cent), alopecia (7 per cent) and pediculosis (5 per cent). The researchers observed use of soap meant for clothes for washing hair. The corrosive action of this soap might be the cause of dandruff, alopecia and other diseases of scalp. Pediculosis (infestation with Pediculus capitis) is picked up through contact with infected persons and may affect the family. Of great importance in the prevention of scalp infestation is daily brushing and combing of hair and a worthy shampoo. Rural ladies instead of undertaking curative measures get such parasites picked up one by one which may not eliminate the disease or infestation.
The skin diseases observed among rural women were boils (9 per cent), dermatitis (8 per cent), scabies (7 per cent), ringworm (3 per cent), and eczema (1 per cent). For want of personal hygiene and clean surroundings, rural women often suffer from these diseases.
The deficiency diseases prevalent among rural women were found to be Vitamin A deficiency (19 per cent), anaemia (5 per cent), osteomalacia (4 per cent) and Vitamin B deficiency (3 per cent). These deficiency diseases are found among people whose dietary intake is not up to the required level. The malnutrition among pregnant women of poor community is widespread. The malnutrition does not result only from poor dietbut also from poor environment6.
Some of the other diseases prevalent among the rural women included headache (55 percent), rheumatism (29 per cent), arthritis (27 per cent), malaria (25 per cent), hysteria (5 per cent), and piles (1 per cent). The high complaint of headache by a majority of rural women need due attention of medical specialists. Nevertheless, headache among most of them could be due to their emotional states resulting possibly from tension and anxiety.
The chi square test indicated to have no significant association between the health problems of rural women and the existence of a government hospital in village.
Constraints in Obtaining Treatment from Government Hospitals
Majority of the rural women (81 per cent) reported that the treatment given in the government hospitals was not effective, and doctor required them to obtain treatment in private c l i n i c s (56 per cent). Some of the other important constraints included were inadequate availability of medicines in hospitals (43 per cent), no availability of medical specialists in hospitals (40 per cent), disease diagnosis not done properly (39 per cent), and expensive treatment (35 per cent).
IMPLICATIONS
Some important implications which the study has brought out are given as under:
1. The rural women were found suffering or had suffered from a number of diseases. This implies that a sizeable number of them are down with one or the other sickness at one time or the other. Undoubtedly, this may be having adverse repercussions on the healthy growth and overall development of rural families. Keeping in view the gravity of this problem, it is quite necessary to revamp the functioning of the existing health services being made available to the rural people in villages so that these are effectively utilized by the target group. The streamlining of the health care facilities and medical services has to be done in a way that the rural women avail themselves of the existing facilities to the maximum possible for promoting not only their health but also of their family.
2. The study has shown that the existence of a hospital or a dispensary in a village has no bearing on the prevalence of diseases among the rural women. Huge amount drawn from public exchequer is invested in establishing hospitals at village level. The absence of relationship between the prevalence of diseases and existence of hospital in a village indicates that these institutions have yet to create an impact of their effective performance in tackling the health problems of the local people. On the one hand supervisory officials should ensure efficient performance of the hospitals and dispensaries, on the other hand they should emphasize on the medical and paramedical staff to develop personal contacts with as many local people as possible so that the available health care facilities are utilized by the maximum number of the local people.
3. Most of the health problems of rural women brought out by the study may be overcome by bringing home to them important and basic information about the causes or causal agents of diseases, transmission of diseases, preventive and control measures, sanitation and hygiene. Therefore, specially designed short duration training programmes tailored to the health needs of the rural women may be organized in villages by the health department. Likewise, camps should be organized in villages by the health department and medical institutions from time to time for providing health check up and treatment facilities at the door steps of the rural people. In these camps medical specialists are invited to provide specialized treatment. This shall also provide opportunities to the specialists to get firsthand experience of the health problems existing in villages.
4. The prevalence of deficiency diseases among rural women is a common feature. To control the wide spread incidence of deficiency diseases among rural women besides concerted educational efforts emphasizing on the need for adequate dietary intake, useful information pertaining to the correct methods of food preparation, healthy life style, utilization of available medical facilities, has to be brought home to the rural people. Educational efforts should not only cover the women folk but also the male members without whose cooperation it may not be feasible to make headway in improving over the existing situation.
5. The constraints, such as, hospital treatment not effective, required by doctors to attend private clinic, lack of medicines in the hospital, etc., indicate almost total neglect of the health problems of the rural women on the part of the authorities concerned. Such type of constraints distracts the concerned clientele from utilizing the available health care facilities. It would be in the public interest to improve the quality of the health care services by diluting the constraints brought out by the study. The planners and policy makers should consider these constraints while planning and formulating health care services and facilities for the rural community.
REFERENCES
1. GUPTA S, SHARMA M.L and DARSHAN S. (1981) Health problems and promotive programmes in rural community - A case study in Haryana. HAU Journal of Research, 11: 1, p. 93-99.
2. SINGH, I.J. (1979) A study of morbidity pattern in rural community. Health and Population - Perspectives and Issues. 2:3, p. 193-206.
3. NAIR, G.R. (1982) The problem villages. Social Welfare. 14:1. p.26-28.
4. RAY. S.K. (1982) Prevalence of dental fluorosis in relation to fluoride In drinking water in two villages of Varanasi (UP.). Indian Journal of Public Health. 26:3, p. 173-178.
5. MAEGRAITH, B. (1974) Diseases due to infection and infestation. In: Price’s Textbook of the Practice of Medicine (ed: R.B. Scott). The English Language Book Society and Oxford University Press, Ely House, London, p. 149-150.
6. GOPALAN, C. (1974) Nutritional problems in India. Social Welfare. 21:1. p.6.
7. Government medical college,Guntur,Andhrapradesh,India.
8. mohfw.nic.in/NRHM/Documents/AP_Facility_Survey_Report.pdf
9. aponline.gov.in/quick%20links/departments/social%20welfare/com missionerate%20of%20social%20welfare/rti%20act/rti_act.html
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE