
{ DOWNLOAD AS PDF }
ABOUT AUTHORS
M.S.Umashankar*1, K.S.Lakshmi, A.Bharath Kumar, A.Porselvi
SRM College of Pharmacy,
SRM University, Kattankulathur,
Tamil Nadu, India
*abharatpharma@gmail.com
ABSTRACT :
It is a critical clinical condition in which more abnormalities in cardiac structure and its functions may impact the ineffectiveness of the heart to supply required oxygen to meet the cellular metabolic demands of the body. Heart is covered with protective layers and express the various functions in the body. Clinically cardiac disease prevalence rises with individual age. Cardiac dysfunction happens because of changes in blood volume, and neurohumoral transmission status. These desirable mechanisms to maintain adequate cardiac output and arterial blood pressure. The neurohumoral responses act as compensatory mechanisms and provokes heart failure by increasing ventricular after load and increasing preload,which further elevates the cardiac failure. Health care system with a clinical pharmacist is well allocated to impact the disease management through identification of risk factors, stage of severity, educating the patients and health care practioners and implementing the awareness programmes, modification of life style interventions with in health care system beneficial to the community may reduce the progression of disease severity.
[adsense:336x280:8701650588]
REFERENCE ID: PHARMATUTOR-ART-2520
|
PharmaTutor (Print-ISSN: 2394 - 6679; e-ISSN: 2347 - 7881) Volume 5, Issue 9 Received On: 04/05/2017; Accepted On: 19/05/2017; Published On: 01/09/2017 How to cite this article: Umashankar MS, Lakshmi KS, Kumar AB, Porselvi A;Clinical Pharmacist specialized care in Management of Congestive Heart Failure - A Brief Review; PharmaTutor; 2017; 5(9); 16-22 |
INTRODUCTION
Congestive heart failure is a clinical syndrome caused by abnormal functional defects in myocardium resulting in impairment of ventricular filling. The hypertension, diabetes mellitus and hyperlipidemia are the major causes of heart failure. The heart is inability to supply oxygen and nutrients to meet the required body needs1. The chambers of the heart contracts to hold more blood to pump through the body.During the heart failure condition heart pumping is weaker. The pressure rises the blood moves slowly from the body to heart. The chambers of the heart may responds to pump the blood to all parts of the body2.
Introduction to Clinical pharmacy
It is defined as area of the pharmacy concerned with science and practice of rational use of drugs. Clinical pharmacists interacts directly with physicians, health professionals and patients to ensure that the medications prescribed for patients contribute to the best possible health outcomes. Clinical pharmacists practice in health care settings where they have frequent and interactions with physicians and other health professionals,contributing to better care3.
The clinical pharmacist is educated and trained in direct patient care wards, including medical centers, clinics and a variety of other health care settings. These privileges are granted on the basis of the clinical pharmacist’s demonstrated knowledge of medication therapy and clinical experience4.
Physiology of heart : The heart is located in the chest between the lungs behind the sternum and above the diaphragm5. It is surrounded by cardiac protective membranes. Its weight is about 250-300 g. It consist of superior and inferior vena cava the pulmonary artery and vein as well as the aorta.
Anatomy of the Heart : The heart walls are composed of cardiac muscles is called myocardium. It consists of four compartments such as the right and left atria and ventricles6. The anterior aspect is the right ventricle and posterior aspect shows the left atrium. The left ventricular walls are much thicker than the right ventricular wall.
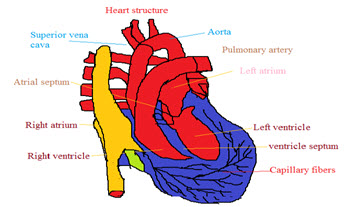
Fig 1 : Structure of Heart
The heart has four valves, the right atrium and ventricle tricuspid valve is present and the left atrium and ventricle mitral valve is located. The pulmonary valve lies between the right ventricle and the pulmonary artery7.
The blood comes back from the systemic circulation to the right atrium and from there moves to tricuspid valve and right ventricle. Oxygenated blood returns from the lungs to the left atrium, and from there moves mitral valve to left ventricle. Finally blood is pumped to the systemic circulation8.
The heart has four chambers.The upper two chambers are the atria and the lower two are the ventricles. The chambers are separated by a wall of tissue called the septum. Blood is pumped through the chambers with the help of four heart valves. The valves open and closed to manage the blood flow in single direction9.
Heart blood flow Patterns :
The normal blood flow is a cyclic process includes Heart moves to Lungs-moves to Heart-finally reaches the Body10.
Right side of the Heart
The right side of the heart receives deoxygenated blood from the body tissues into the right atrium. This deoxygenated blood passes through the tricuspid valve into the right ventricle.
Left side of the Heart
The left-hand side of the heart receives oxygenated blood from the lungs into the left atrium. This oxygenated blood then passes through the bicuspid valve into the left ventricle11.
Risk Factors
The main risk factors for congestive heart failure are :
|
High blood pressure |
Coronary heart disease |
|
Diabetes |
Valve defects13 |
|
Heart attack |
Viral or bacterial infection |
|
Obesity |
Alcohol, Drugs, Tobacco |
|
Decreased kidney function |
COPD |
|
High cholesterol12 |
Asthma13 |
Pathophysiology
The decrease in heart rate causes reduced cardiac out put which causes the myocardial injury. Improper regulation of baro receptor stimulations causes the irregular heart pulses15. The reduced left ventricular function and activation of renin angiotensin aldosterone system causes more vasoconstriction and altered hemodynamic activity which causes the improper regulation of left ventricular function14.
The activation of renin angiotensin aldosterone system the angiotensin 1 is converted to angiotensin II causes the severe vasoconstriction16. The aldosterone secretion causes the salt and water retension increase the plasma volume and increase the preload, after load and cardiac work load consequences causes the heart failure.
Tests and diagnosis
Blood tests : Sample of blood is collected from patient to check the any infections, inflammations,look of indicators for other diseases that affect the heart17.
Chest X-ray : The presence of heart failure, the heart may appear enlarged and more fluid deposition in the lungs.
Electrocardiogram : This test records the electrical activity of heart. The electrodes attached to skin. The Impulses are recorded as waves and displayed on a paper18.
Echocardiogram : An echocardiogram uses sound waves to produce a video image of heart. This test can help the physicians to verify the size and shape,pumping effectivenss of heart19.
Cardiac computerized tomography (CT) scan and magnetic resonance imaging (MRI): This test can be used to investigate the physiological process,anatomical positions of the working status of the heart to diagnose heart problems.
Coronary angiogram : In this test a thin, flexible catheter is inserted into a blood vessel at groin and guided through the aorta into coronary arteries20.
Myocardial biopsy : In this test inserting a small, flexible biopsy cord into a vein in neck or and a small pieces of the heart muscle is taken21.
Doppler Imaging : This test uses sound waves to measure the speed and direction of blood flow and valvular function.
Holter Monitor: A holter monitor is a small box and is attached to electrodes that are placed on chest which records the rhythm of heart.
Cardiac Magnetic Resonance Imaging (MRI) : An MRI shows the structure and beating capability,contractions of heart and signs of damage.
Positron Emission Tomography : It is used to see the blood is flow to the heart22.
Thyroid Function Tests : This test is performed to determine the causes of heart failure due to thyroid dysfunction.
Symptoms
|
Weakness |
Swelling of feet |
|
feeling tired |
Changes in the frequency of urination |
|
coughing |
Severe shortness of breath. |
|
Weight gain |
Profuse sweating,Chest pain23 |
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
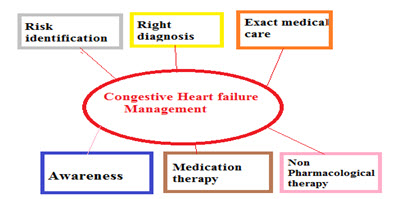
Clinical pharmacist intervention in management of congestive cardiac failure :
• Eating a healthy and balanced diet : Choosing nutrient-rich foods which have vitamins, minerals, fiber and other nutrients but are lower in calories over nutrient-poor foods.
• Eating diet containing low in salt, fat, saturated fat, trans fat and cholesterol.
• Monitoring the salt intake.
• Reducing the cholesterol levels in body.
• Weight reduction practices.
• Regular physical activity24
Avoiding the alcohol habbit :
• Drinking too much alcohol can raise blood pressure, increase cardiomyopathy, stroke, cancer, and other diseases. It can contribute to high triglycerides and produce irregular heartbeats. Excessive alcohol consumption contributes to obesity, alcoholism, suicide and accidents.
• Avoiding the smoking habbit25.
• Getting adequate relaxed sleep.
• Maintaining the low sodium diet.
• Exercising regularly.
• Strict Medication adherence.
• Stress management26.
Treatment for congestive heart failure
Drugs : A variety of medicines are available to help and treat congestive heart failure. Some of the most frequently prescribed medications include:
Angiotensin Converting Enzyme (ACE) Inhibitors
Commonly prescribed include:
• Captopril , Enalapril, Fosinopril, Lisinopril ,Perindopril, Quinapril, Ramipril
• Benazepril: Usual dose : 20-40 mg in a single or 2 divided doses.
• Captopril: Congestive heart failure / Hypertension : 6.25-12.5 mg three times a day.
• Enalapril: Congestive heart failure / Hypertension : 2.5-5 mg daily increased up to 40 mg/day.
• Fosinopril: Usual dose : 20-40 mg daily.
• Lisinopril: Dose range : 10-40 mg daily.
• Ramipril: Hypertension : 2.5-5 mg once daily.
• Trandolapril : 1 mg/day.
Angiotensin II Receptor Blockers
Commonly prescribed include : Valsartan, Losartan, Candesartan,Valsartan, Telmisartan, Irbesartan27.
Candesartan : 4 mg, 8 mg, 16 mg, 32 mg
Irbesartan : 75 mg, 150 mg, 300 mg
losartan: 25 mg, 50 mg, 100 mg
Telmisartan : 20 mg, 40 mg, 80 mg
valsartan : 40 mg, 80 mg
Beta Blockers
Commonly prescribed include:
•Bisoprolol, Metoprolol, propranolol, metaprolol, atenolol, acebutalol, esmolol, timolol.
|
Acebutolol 200 mg |
Carvedilol 25 mg |
Nadolol 80 mg |
|
Atenolol 50 mg |
Labetalol 200 mg |
Pindolol 7.5 mg |
|
Bisoprolol 5 mg |
Metoprolol 100 mg |
Propranolol 80 mg |
Side effects : Rashes, Tachycardia, Weakness, Nausea, Vomiting, Abdominal discomfort.
Aldosterone Antagonists
Commonly prescribed drugs include : Spironolactone, Eplerenone.
Diuretics Commonly prescribed include:
|
Furosemide (Lasix) |
Chlorothiazide |
Indapamide |
|
Bumetanide |
Amiloride |
Metolazone |
|
Torsemide |
Hydro chlorothiazide |
Triamterene |
Furosemide dosing information : Dose : 20 mg - 80 mg.
Adverse effects : Sudden weakness, Electrolyte imbalance , kidney problems , Severe skin reactions28.
Spironolactone dosing information
• Usual Adult Dose for Edema:
• 25 to 200 mg/day orally in 1 or 2 divided doses.
• Usual Adult Dose for Hypertension:
• 25 to 200 mg/day orally in 1 or 2 divided doses.
• Usual Adult Dose for Hypokalemia:
• 25 to 200 mg/day orally in 1 or 2 divided doses.
• Usual Adult Dose for Primary Hyperaldosteronism Diagnosis:
• 100 to 400 mg/day orally in 1 or 2 divided doses.
• Usual Adult Dose for Hirsutism:
• 50 to 200 mg/day orally in 1 or 2 divided doses.
• Usual Adult Dose for Congestive Heart Failure:
• 25 mg/day orally.
Adverse effects : lower back or side pain,lump in the breast or under the arm, muscle pain or cramps,muscle spasms or twitching.
Vasodilators :
Isosorbide dinitrate : 20 mg three times a day.
Hydralazine : 37.5 mg three times a day.
Side Effects of vasodilators may include:
Chest pain, Heart palpitations, Rapid heart beat, Fluid retention, Nausea, vomiting, Dizziness and Headache.
Other medications that might be prescribed includes :
These drugs include : Digoxin : Dosage Forms & Strengths.oral solution : 0.05mg/mL , injectable solution : 0.1mg/mL.
Atrial Fibrillation
Rapid digitalizing regimen : IV : 8-12 mcg/kg (0.008-0.012 mg/kg) total loading dose.PO : 10-15 mcg/kg total loading dose.
Maintenance : PO : 3.4-5.1 mcg/kg/day or 0.125-0.5 mg/day PO.IV/IM : 0.1-0.4 mg q Day.
Heart Failure ; 0.125-0.25 mg PO/IV q Day.
Adverse effects : Nausea, vomiting, diarrhea, loss of appetite, weakness, dizziness, headache, anxiety, depression, bradycardia, skin rash.
Surgery and medical devices for congestive heart failure treatment
In few cases the patient is recommend for surgery to treat the underlying problem that led to heart failure. It includes :
Coronary bypass surgery :
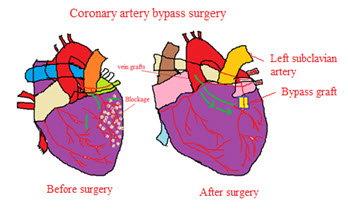
Fig 3 : Before and After changes in Coronary bypass surgery
• Coronary bypass surgery is a surgical procedure that diverts the flow of blood around a section of a blocked artery in heart. By creating a new pathway to the heart, coronary bypass surgery improves blood flow to cardiac muscle29.
• During coronary bypass surgery, a healthy blood vessel is taken from legs, chest connected to the other arteries in heart so that blood bypasses the diseased site.
• After coronary bypass surgery, symptoms, such as chest pain and shortness of breath due to poor blood flow to the heart, generally improved.
Heart valve replacement : Valve repair can usually be done on congenital valve defects and has a good success record with treating mitral valve defects. Severe valve damage consequences valve must be replaced includes aortic or mitral valve.
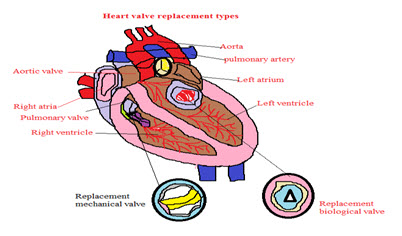
Fig 4 : Heart valve replacemen
Two kinds of valves can be used for replacement:
•Mechanical valves are usually made from plastic, carbon, or metal. Mechanical valves are strong, and they last a long time.
• Biological valves are made from animal tissue and taken from the human tissue of a donated heart known as allograft or homograft. Biological valves break down faster in children and young adults, these valves are used often in elderly patients.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Implantable cardioverter-defibrillators : An ICD is a device similar to a pacemaker. It's implanted under the skin present in chest with wires in veins and into heart. The ICD monitors the heart rhythm.

Fig 5 : Implantable cardioverter-defibrillators
Cardiac resynchronization therapy (CRT), or biventricular pacing. A biventricular pacemaker sends timed electrical impulses to both of the heart's lower chambers (the left and right ventricles) so that they pump in a more efficient, coordinated manner.
Heart pumps : These mechanical devices, such as ventricular assist devices are implanted into the chest and attached to a weakened heart to pump blood to the rest of the body.
Heart transplant : Heart transplants can dramatically improve the survival and quality of life of some people with severe heart failure30.
Device therapy : Inserting a biventricular pacemaker known as cardiac resynchronisation therapy, may restore synchrony to the ventricles.
Implantable cardiac defibrillators (ICDs): It pevents the sudden cardiac death by delivering an electric shock to the heart to stop the ventricular arrhythmia and restore the heart to a normal rhythm.
CONCLUSION
The clinical pharmacist having significant role in life style interventions may impact reducing the cardiac health problems in patients with heart failure. The effective implementing treatment at early stages of the disease condition may improve the better health status in individual patients with heart failure30. These approaches are beneficial to the patients to minimize the hospital admissions in future.
The prevention of disease depends on identification of causative factors, early screening of high risk patients, diagnosis and life style intervention practices may beneficial. The management of disease depends on reaching the various pharmacological classes of medications and surgical treatment available to manage the cardiac diseases and effective medication adherence practices may reduce the disease burden.
Heart failure is a complex clinical syndrome the diagnosis depends on various symptoms and laboratory investigations. The First-line pharmacotherapy consists of angiotensin converting enzyme inhibitors and β-blockers. The recent treatment depends on implantable cardioverter defibrillators and cardiac resynchronisation therapies are strongly recommended.
Community level awareness programmes will efforts at risk factor identification and its prevention. The adoption of healthy lifestyle habbits in individual patients essential to promote better outcomes and deflate the heart failure.
REFERENCES
1. Hobbs FDR. The scale of heart failure: diagnosis and management issues for primary care. Heart. 1999;82(Suppl. IV):8–10.
2. Mahoney JS. An ethnographic approach to understanding the illness experiences of patients with congestive heart failure and their family members. Heart Lung. 2001;30:429–36.
3. Sullivan MJ, Hawthorne MH. Nonpharmacological interventions in the treatment of heart failure. J Cardiovasc Nurs. 1996;10:47–57.
4. Carlson B, Riegel B, Faan C, Moser D. Self-care abilities of patients with heart failure. Heart Lung. 2001;30:351–9.
5. Zannad F. Evidence-based drug therapy for chronic heart failure. Eur Heart J. 2002;(Suppl. 4):D66–D72.
6. Varma S, McElnay JC, Hughes CM. A qualitative assessment of health-related issues of importance in elderly congestive heart failure patients. J Soc Admin Pharm. 2001;18:59–67.
7. Murray SA, Boyd K, Kendall M, Worth A, Benton TF, Clausen H. Exploring the spiritual needs of people dying of lung cancer or heart failure: a prospective qualitative interview study of patients and their carers. BMJ. 2002;325:929–33.
8. Rogers A, Addington-Hall JM, McCoy ASM, Edmonds PM, Abery AJ, Coats AJS, Gibbs JSR. A qualitative study of chronic heart failure patients' understanding of their symptoms and drug therapy. Eur J Heart Fail. 2002;4:283–7.
9. Martensson J, Karlsson J, Fridlund B. Male patients with CHF and their conception of the life situation. J Adv Nurs. 1997;25:579–86.
10. Sneed N, Paul S, Michel Y, VanBakel A, Hendrix G. Evaluation of three quality of life measurement tools in patients with chronic heart failure. Heart Lung. 2001;30:332–40.
11. Dracup K, Baker DW, Dunbar SB, Dacey RA, Brooks NH, Johnson JC, Oken C, Massie BM. Management of heart failure. Counselling, education, and lifestyle modifications. JAMA. 1994;272:1442–6.
12. Coats AJS. What causes symptoms in heart failure? Heart. 2001;86:574–8.
13. Hepler CD, Strand L. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47:533–43.
14. Stewart S, Pearson S, Horowitz JD. Effects of a home-based intervention among patients with congestive heart failure discharged from acute hospital care. Arch Intern Med. 1998;158:1067–72.
15. Varma S, McElnay JC, Hughes CM, Passmore AP, Varma M. Pharmaceutical care of elderly congestive heart failure patients: Interventions and outcomes. Pharmacoth. 1999;19:860–9.
16. Gattis WA, Hasselbad V, Whellan DJ, O'Connor CM. Reduction in heart failure events by the addition of a clinical pharmacist to the heart failure management team — Results of the Pharmacist in Heart Failure Assessment Recommendation and Monitoring (PHARM) Study.Arch Intern Med. 1999;159:1939–45.
17. Luzier AB, Forrest A, Feuerstein SG, Schentag JJ, Izzo JL. Containment of heart failure hospitalizations and cost by angiotensin-converting enzyme inhibitor dosage optimization. Am J Cardiol. 2000;86:519–23.
18. Pearson GJ, Cooke C, Simmons WKT, Sketris I. Evaluation of the use of evidence-based angiotensin-converting enzyme inhibitor criteria for the treatment of congestive heart failure: opportunities for pharmacists to improve patient outcomes. J Clin Pharm Ther. 2001;26:351–61.
19. Stewart S, Marley J, Horowitz J. Effects of a multidisciplinary, home based intervention on unplanned readmissions and survival among patients with chronic congestive heart failure: a randomized controlled study. Lancet. 1999;354:1077–83.
20. Gore S. Assessing clinical trials-restricted randomisation. BMJ. 1981;282:2114–7.
21. Cohn SR, Mount MM, Tomas JJ, Mount LF. Existential well-being is an important determinant of quality of life. Cancer. 1996;77:567–86.
22. Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three decades of research. A comprehensive review. J Clin Pharm Ther. 2001;26:331–42.
23. Centre for Health Protection, Department of Health, The Government of HKSAR. Number of Deaths by Leading Causes of Death by Sex by Age in 2011. 2012.
24. Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Katz SD, et al. Executive summary: HFSA 2010 comprehensive heart failure practive guideline. J Card Fail. 2010;16:475–539.
25. Bertoni AG, Hundley WG, Massing MW, Bonds DE, Burke GL, Goff DC. Heart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care. 2004;27(3):699–703.
26. Gustafsson F, Arnold JM. Heart failure clinics and outpatient management: review of the evidence and call for quality assurance. Eur Heart J 2004;25:1596–1604
27. Roberts F, Ryan GJ: The safety of metformin in heart failure. Ann Pharmacother 41:642, 2007.
28. Mariani M, Vella G, Bianchi C, Verde S, De MR, Pirelli S. Implementation of beta-blockade in elderly heart failure patients: role of the nurse specialist. Eur J Cardiovasc Nurs 2008;7:196–203.
29. Lainscak M, Farkas J. Challenges of beta blocker therapy in chronic heart failure: the story continues. Eur J Cardiovasc Nurs 2008;7:159–160.
30. Jaarsma T. Health care professionals in a heart failure team.Eur J Heart Fail 2005;7:343–349.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT editor-in-chief@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE








