

 About Authors:
About Authors:
Kalyan K Sarkar*1, Dr.Gouranga Das2
1B.Pharm student of 2011 at Institute of Pharmacy,
Govt. Of West Bengal,Jalpaiguri
2,Lecturer,Institute of Pharmacy,Govt of West BengalJalpaiguri
*kalyankrsarkar@gmail.com
ABSTRACT:
A hospital based prospective study was carried out on the patients who were admitted in the surgical and medical in-patients department (IPD) of that therapeutic care unit atJ alpaiguri, West Bengal. Only willing patients were included in our study. Question series was prepared for patient's interview which include age, sex, disease conditions, generic name, brand name of the anti ulcer drugs used and total cost of medication on our study period. The main objective of this study was to find out the actual sketch related to use of anti ulcer drugs in recent days. And finally In our study we have found that patients with various disease such as cardio vascular disease, abdominal pain, abnormal vomiting etc. were given anti ulcer drugs with main medication.
[adsense:336x280:8701650588]
Reference Id: PHARMATUTOR-ART-1388
INTRODUCTION:
Anti Ulcer Drugs are the medicines used to treat ulcers of upper gastrointestinal tract. Ulcers are sores or raw areas that form in the lining of the stomach or the duodenum (the upper part of the intestine). The ulceration of stomach is gastric ulcer.If the ulcer is present then it is duodenal Ulcers. Both types of ulceration are referred to as Peptic Ulcers.The most common cause of ulcer is caused either by infection with a bacterium called Helicobacter Pylori or by long-term use of aspirin or other Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). In either case, something damages the barrier of mucus that normally protects the stomach and duodenum from the powerful acids and enzymes that the body produces to digest food. When that happens,the acids and enzymes begin to eat away the unprotected tissue, causing ulcer.
[adsense:468x15:2204050025]
Rationalization : More than 75% of critically ill patient develop stress induced ulcer within 24 hour of admission to an ICU. Both central and peripheral mechanisms are involved in stress induced ulceration .
There are four possible mechanisms through which the centrally initiated stimuli may cause gastric ulceration
·Increased parasympathetic outflow along vagus.
·Increased outflow of impulses through sympathetic nerves.
·Increased discharge of catecholamines from adrenal medulla.
·Activation of the pituitary adrenal axis leading to a discharge of adrenal cortico steroids.
On the other hand the peripheral pathways stress induced ulceration is the vagus and the sympathetic outflow. If the restraint is combined with cold (4 degree centigrade) the ulcer is hastened. The plasma concentration of histamine is seen high in restraint ulceration. Further the concentration of the stress hormone Angictensin II (ANG II) dramatically increases in plasma, tissue and stomach. ANG II constricts the gastric vascular through AT receptor stimulation followed by the increased gastric blood flow. In addition ANG II generates reactive oxygen species with cellular damage and inflammation. Reactive oxygen species stimulate the nuclear factor kB (NF-kB) to produce pro-inflammatory cytokines which damage the mucosal cells by inflammatory pathway (Claudia B et. Al., 2003). In a study it was seen that ethanol induced LTC4 production causes the static of gastric blood flow following vasoconstriction in both venus and arterial vessels. 5-Lipoxygenase metabolic products of archidonic acid act on mucosal mast cell to release histamine followed by ulceration. This kind of ulceration increases the length of ICU stay by 4-8 days resulting in the increase of treatment cost and is associated with an increased mortality rate. In such cases prophylactic therapy with anti-ulcer drug is reccomended to prevent the bleeding.
Patient at risk for stressed induced ulcer include those with respiratory failure, coagulopathy, hypertention, sepsis, hepatic failure, acute renal failure,multiple trauma,severe burn,head injury, traumatic spinal cord injury, major surgery or history of gastrointestinal bleeding (Cook DJ et. Al., 1994).
Therapeutic options for the presentation of the stress related mucosal bleeding include antacids, H2RAs, PPIs and sucralfate.Continuous intravenous infusion of cimetidine is the only regimen that is FDA labeled for the prevention of SRMB. However, H2 receptor blockers are preferred for the prophylaxis of SRMB. Intravenous ranitidine is superior for sucralfate in preventing stress related mucosal bleeding (Cook D et. Al., 1998). PPIs can also be used as an alternative.
In our study we have studied the use of antiulcer drugs in the surgical and medical inpatient department of a tertiary care unit of the district , Jalpaiguri. The objective of our study was to check that whether the theraputic care unit is following proper guideline to use the common antiulcer drugs as prophylaxis therapy or not.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
MATERIALS AND METHOD:
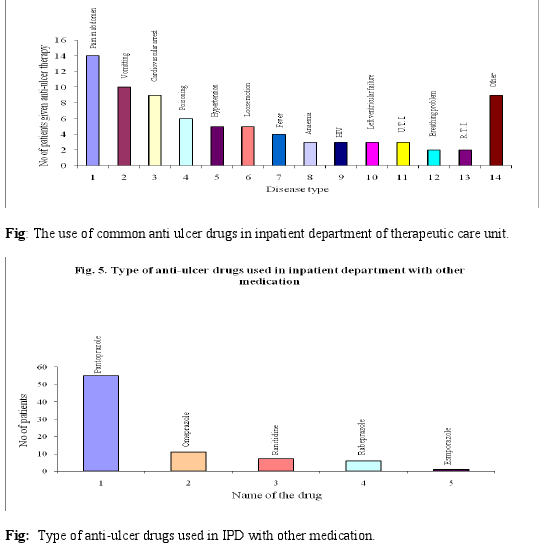
This study was undertaken in the surgical and medical department of the theraputic care unit at jalpaiguri,West Bengal as per proper authorization. only wiling patients are included in our study,some questionares were prepared for patient’s interview which include age, sex disease condition, genetic name, brand of antiulcer drugs used and total cost of medication.Our study was conducted on 80 patients (given anti-ulcer therapy) of surgical and medical inpatient department, Table. 1. represents the category of disease where the anti ulcer drugs were given to patients along with main medication. Table. 2. represents the use of common anti ulcer drugs in medical and surgical inpatient departments.
|
Disease type |
No. of patients given anti-ulcer therapy with main therapy |
|
Pain in Abdomen |
14 |
|
Vomiting |
10 |
|
Cardiovascular arrest |
9 |
|
Poisoning |
6 |
|
Hypertension |
5 |
|
Loose motion |
5 |
|
Feever |
4 |
|
Anaemia |
3 |
|
HIV |
3 |
|
Left ventricular failure |
3 |
|
Urinary tract infection (U. T. I.) |
3 |
|
Breathing Problem |
2 |
|
Respiratory tract infection (R. T. I.) |
2 |
|
Others |
9 |
Table. 1. Category of disease where the anti ulcer drugs were given to patients.
|
Name of the drugs |
No. of patients |
|
1. Pantoprazole |
55 |
|
2. Omeprazole |
11 |
|
3. Ranitidine |
7 |
|
4. Rabeprazole |
6 |
|
5. Esomopeazole |
1 |
Table. 2. Common anti ulcer drugs in medical and surgical inpatient departments.
RESULTS AND DISSCUTIONS:
From our study we have evaluated that patients with abdominal pain, vomiting. Cardiovascular disorders, poisoning etc were given anti ulcer drugs with main medication.Most of them were given proton pump inhibitors (Pantoprazole and omeprazole). However some paients were also given ranitidine, the H2 blocker.
The use of common anti ulcer drug in hospital is not as per the rational guideline. Conversely all proton pump inhibitors show same efficacy as prophylactic therapy and can be used as prophylactic anti-ulcer drug in ICU or other inpatient department. However more sample size is required to draw the final conclusion.
REFERENCES:
• Cook D et. Al.American society of health system pharmacists therapeutic guideline on stress ulcer prophylaxis. Am J Health system pharm.1999.56:347-379
• Bhargava KP, Das M, Gupta GP, Gupta MB. Study of contral neurotransmitters in strens induced gastric ulceration in albino rats. Br J. pharmacy 1980. 68:765-772.
• Claudia B, Ines A, Hiremichi A.et. al. Anti-inflammatory effects of angiotensin II (AT2) receptor antagonism prevent stress induced gastric injury. Am J Physol Gastrointest Physiol. 2003. 285:4414-4423.
• Cook D, Guyatt G, Marshall J et.al,A comparison of sucralfate and ranitidine for prevention of upper gastro intestinal bleeding in patients requiring mechanical ventilation.N Eng J med.1998.338:791 -797.
• Cook D, Heyland D,Grffith L-Et . al. Risk factors for clinically important upper gastro intestinal bleeding in patients requiring mechanical ventilation.crit care med.1999.27:2812-2817.
• Cook DJ, Fulla HD,Guyatt GH et. Al.Risk factors for gastrointestinal bleeding in coitically ill patients.N Ebgl J Med.1994. 330:377-381.
• Dippiro JT, Talbert RL, Matzke GR et. al. Pharmacotherapy A pathologic approach. Mc. graw hill. 6th edition. 2007. 613-648.
• Tripathi KD. Essential of medical pharmacology.jaypee.2008.627-634.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE






