
About Author: Ram Ashwin
Peptic Ulcer Disease and its screening
Condition characterized by Erosion of GI mucosa resulting from digestive action of HCl and pepsin or A peptic ulcer is erosion in the lining of the stomach or the first part of the small intestine, an area called the duodenum.
• Ulcer development
• Lower esophagus(esophageal ulcer)
• Stomach(gastric ulcer)
• Duodenum(duodenal ulcer)
[adsense:336x280:8701650588]
Reference ID: PHARMATUTOR-ART-1102
Types
• Acute
• Superficial erosion
• Minimal erosion
• Chronic
• Muscular wall erosion with formation of fibrous tissue
• Present continuously for many months or intermittently
Peptic Ulcer Disease Etiology and Pathophysiology
• Develop only in presence of acid environment
• Excess of gastric acid not necessary for ulcer development
• Person with a gastric ulcer has normal to less than normal gastric acidity compared with person with a duodenal ulcer
• Some intraluminal acid does seem to be essential for a gastric ulcer to occur
• Pepsinogen is activated to pepsin in presence of HCl and a pH of 2 to 3
• Secretion of HCl by parietal cells has a pH of 0.8
• pH reaches 2 to 3 after mixing with stomach contents
• At pH level 3.5 or more, stomach acid is neutralized
• Pepsin has little or no proteolytic activity
• Surface mucosa of stomach is renewed about every 3 days
• Mucosa can continually repair itself except in extreme instances
• Mucosal barrier prevents back diffusion of acid from gastric lumen through mucosal layers to underlying tissue
• Mucosal barrier can be impaired and back diffusion can occur
[adsense:468x15:2204050025]
PHYSIOLOGY OF ACID SECRETION
The parietal cell contains receptors for gastrin, histamine (H2), and acetylcholine (muscarinic, M3)
When acetylcholine or gastrin bind to the parietal cell receptors, they cause an increase in cytosolic calcium, which in turn stimulates protein kinases that stimulate acid secretion from a H+/K+ ATPase (the proton pump) on the canalicular surface.
In close proximity to the parietal cells are gut endocrine cells called enterochromaffin-like (ECL) cells. ECL cells have receptors for gastrin and acetylcholine and are the major source for histamine release. Histamine binds to the H2 receptor on the parietal cell, resulting in activation of adenylyl cyclase, which increases intracellular cyclic adenosine monophosphate (cAMP). cAMP activates protein kinases that stimulate acid secretion by the H+/K+ ATPase. In humans, it is believed that the major effect of gastrin upon acid secretion is mediated indirectly through the release of histamine from ECL cells rather than through direct parietal cell stimulation.
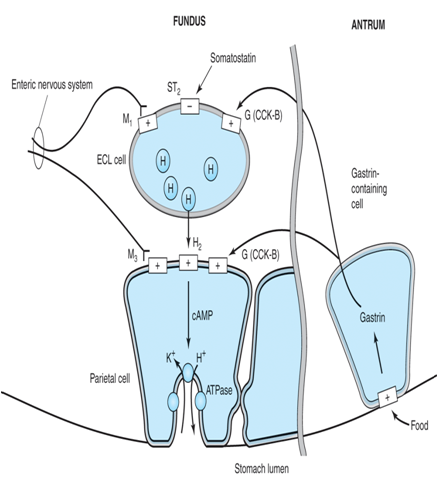
Schematic diagram of one model of the physiologic control of hydrogen ion secretion by the gastric parietal cell. ECL cell, enterochromaffin-like cell; G(CCK-B), gastrin-cholecystokinin-B receptor; H, histamine; H2, histamine H2 receptor; M1, M3, muscarinic receptors; ST2, somatostatin-2 receptor; ATPase, H+/K+ ATPase proton pump.
Back Diffusion of Acids Fig.
Peptic Ulcer Disease Etiology and Pathophysiology
• HCl freely enters mucosa when barrier is broken
• Injury to tissue occurs
• Result: cellular destruction and inflammation
• Histamine is released
• Vasodilation, ↑ capillary permeability
• Further secretion of acid and pepsin
• Ulcerogenic drugs inhibit synthesis of prostaglandins and cause abnormal permeability
• Corticosteroids ↓ rate of mucosal cell renewal thereby ↓ protective effects
• When mucosal barrier is disrupted, there is a compensatory ↑ in blood flow
• Prostaglandin-like substances, histamines act as vasodilators
• Hydrogen ions are rapidly removed
• Buffers are delivered
• Nutrients arrive
• Mucosal cell replication
• When blood flow is not sufficient, tissue injury results
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Disruption of Gastric Mucosal Barrier
Two mechanisms that protect
• Mucus forms a layer that entraps or slows diffusion of hydrogen ions across mucosal barrier
• Bicarbonate is secreted
• Neutralizes HCl acid in lumen of GI tract
• Vagal nerve stimulation results in hypersecretion of HCl acid
• HCl acid can alter mucosal barrier
• Duodenal ulcers are associated with acid
Peptic Ulcer Disease Clinical Manifestations
• Common to have no pain or other symptoms
• Gastric and duodenal mucosa not rich in sensory pain fibers
• Duodenal ulcer pain
• Burning, cramplike
• Gastric ulcer pain
• Burning, gaseous
• 3 major complications
• Hemorrhage
• Perforation
• Gastric outlet obstruction
Peptic Ulcer DiseaseHemorrhage
• Most common complication of peptic ulcer disease
• Develops from erosion of
• Granulation tissue found at base of ulcer during healing
• Ulcer through a major blood vessel
• Occurs when ulcer penetrates serosal surface
• Spillage of their gastric or duodenal contents into peritoneal cavity
• Size of perforation directly proportional to length of time patient has had ulcer
• Sudden, dramatic onset
Peptic Ulcer Disease Gastric Outlet Obstruction
• Ulcers located in antrum and prepyloric and pyloric areas of stomach
• Duodenum can predispose to gastric outlet obstruction
• contractile force needed to empty stomach results in hypertrophy of stomach wall
• Peptic Ulcer DiseaseGastric Outlet Obstruction
• After longstanding obstruction stomach enters decompensated phase
• Results in dilation and atony
• Obstruction is not totally due to fibrous scar tissue
• Active ulcer formation is associated with edema, inflammation, pylorospasm
• All contribute to narrowing of pylorus
• Usually has a history of ulcer pain
• Short duration or absence of pain indicative of a malignant obstruction
• Vomiting is common
• Constipation is a common complaint
• Dehydration, lack of roughage in diet
• May show swelling in upper abdomen
Peptic Ulcer Disease Diagnostic Studies
• Endoscopy procedure most often used
• Determines degree of ulcer healing after treatment
• Tissue specimens can be obtained to identify H. pyloriand to rule out gastric cancer
• Tests for H. pylori
• Noninvasive tests
• Serum or whole blood antibody tests
• Immunoglobin G (IgG)
• Urea breath test
• Invasive tests
• Biopsy of stomach
• Rapid urease test
• Barium contrast studies
• Widely used
• X-ray studies
• Ineffective in differentiating a peptic ulcer from a malignant tumor
• Gastric analysis
• Identifying a possible gastrinoma
• Determining degree of gastric hyperacidity
• Evaluating results of therapy
• Laboratory analysis
• CBC
• Urinalysis
• Liver enzyme studies
• Serum amylase determination
• Stool examination
Peptic Ulcer Disease Collaborative Care
Medical regimen consists of
• Adequate rest
• Dietary modification
• Drug therapy
• Elimination of smoking
• Long-term follow-up care
• Aim of treatment program
• degree of gastric acidity
• Enhance mucosal defense mechanisms
• Minimize harmful effects on mucosa
• Generally treated in ambulatory care clinics
• Requires many weeks of therapy
• Pain disappears after 3 to 6 days
Healing may take 3 to 9 weeks
• Should be assessed by means of x-rays or endoscopic examination
• Moderation in daily activity is essential
• NSAIDs that are COX-2 inhibitors are used
Peptic Ulcer Disease Drug Therapy
Includes use of
• Antacids
• H2R blockers
• PPIs
• Antibiotics
• Anticholinergics
• Cytoproctective therapy
Recurrence of peptic ulcer is frequent
• Interruption or discontinuation of therapy can have detrimental results
• No drugs, unless prescribed by health care provider, should be taken
• Ulcerogenic effect
Histamine-2 receptor blocks (H2R blockers)
• Used to manage peptic ulcer disease
• Block action of histamine on H2receptors
• Decrease HCl acid secretion
• Decrease conversion of pepsinogen to pepsin
• Increase ulcer healing
Proton pump inhibitors (PPI)
• Block ATPase enzyme that is important for secretion of HCl acid
Antibiotic therapy
• Eradicate H. pyloriinfection
• No single agents have been effective in eliminating H. pylori
Antacids
• Used as adjunct therapy for peptic ulcer disease
• Increase gastric pH by neutralizing acid
Anticholinergic drugs
• Occasionally ordered for treatment
• Decrease cholinergic stimulation of HCl acid
Cytoprotective drug therapy
• Used for short-term treatment of ulcers
• Tricyclic antidepressants
• Serotonin reuptake inhibitors
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Peptic Ulcer DiseaseNutritional Therapy
• Dietary modifications may be necessary so that foods and beverages irritating to patient can be avoided or eliminated
• Nonirritating or bland diet consisting of 6 small meals a day during symptomatic phase
• Include a sample diet with a list of foods that usually cause distress
• Hot, spicy foods and pepper, alcohol, carbonated beverages, tea, coffee, broth
• Foods high in roughage may irritate an inflamed mucosa
• Protein considered best neutralizing food
• Stimulates gastric secretions
• Carbohydrates and fats are least stimulating to HCl acid secretion
• Do not neutralize well
• Milk can neutralize gastric acidity and contains prostaglandins and growth factors
• Protects GI mucosa from injury
SCREENING METHODS
Screening Methods in Pharmacology provides an up to-date and concise account of in vivo methods used in the pharmacological screening of important categories of clinically useful drugs. It also encompasses the basic principles of animal experimentation and current advances leading to the use of transgenic animals, combinatorial chemistry, high throughout screening, pharmacogenomics, proteomics and array technology. The methods used for the detection of pharmacological effects of potential drugs on the CNS, CVS, endocrines, respiratory tract and immunomodulation have been described in adequate details with cross references for further studies and comprehension.
ORGANIZATION OF SCREENING
SCREENING OF DRUGS INVOLVES
scanning permits detection of physiological activity.
If scanning results are not very sure, then go for evaluation.
• There are three kinds of screening of pharmaceuticals, the distinction lying in the different aims of screening scanning
• evaluation
• simple screening
• blind screening
• programmed screening
A) SIMPLE SCREENING
• when one or two tests are used to find substances having a particular activity, the screening is simple.
Eg:- single test for the concentration of sugar in the blood might be used to screen compounds for hypoglycemic activity
B) Blind Screening
when a new drug is available (either from natural or synthetic source) and there may be no information on its pharmacological activity, then we go for blind screening
blind screening provides clues to
• potential activity
• fields of activity
• pharmacological inertness, if it exists
C) PROGRAMMED SCREENING
As the name suggests, a programme of testing is required to provide information on the compounds, that only a series of tests can provide.
Merits:-
1. greater precision in the result
2. Indicates potential side effects
3. Detailed pharmacology of the most promising substances
SCREENING METHOD OF ANTIULCER DRUG
> PYLORUS LIGATION IN RATS (SHAY RAT).
> STRESS ULCER THROUGH IMMOBILIZATION STRESS.
> STRESS ULCERS BY COLD WATER IMMERSION.
> INDOMETHACIN INDUCED ULCERS IN RATS. (CYTOPROTECTIVE ACTIVITY).
> ETHANOL INDUCED MUCOSAL DAMAGE IN RATS
> SUBACUTE GASTRIC ULCER IN RATS.
> GASTRIC ISCHEMIA-REPERFUSION IN RATS.
CAUSES OF ULCER
Gastric ulcers are caused due to imbalances between aggressive and defensive factors of the gastric mucosa.
AGGRESSIVE FACTOR:
> Increased acid secretion
> Increased pepsin secretion.
> Helicobacter pylori infection
> Decreased mucosal secretion.
DEFENSIVE FACTOR:
> Mucous secretion that forms the protective covering
> Constant cell repairing
> Prostaglandin secretion
> Increased blood flow to gastric mucosa
> Smoking, alcohol, stress.
SOME OTHER FACTOR
Use of NSAIDS, smoking, increase age
Ibuprofen, nicotine, caffeine and alcohol, Red chilly
Chewing tobacco, spicy food, stress etc.
DRUG FOR PEPTIC ULCER
1. Reduction of Gastric acid secretion-
> H2-antihistamine:-Ranitidine, Famotidine etc.
> Proton pump inhibitor:- Omeprazole, Lansoprazole etc.
> Anticholinergics:- pirenzipine, propantheline.
> Prostaglandin analogues:- Misoprostal, Rioprostil,
2. Neutralization of gastric acid (ANTACIDS)-
> Systemic :- Sodium bicarbonate, Calcium carbonate
> Non - systemic:- magnesium hydroxide, aluminiumhydraoxide gel
3. Ulcer Protective- Sucralfate, Bismuth sub citrate.
4. Promoter of Ulcer healing- Carbinoxalone sodium.
5. Anti-H.Pylori drug- Amoxicillin, Clarithromycin, Tetracycline, Tinidazole.
NOTE- The most prescribed drug now a days is an antiulcer drug (Ranitidine).
• Three pathways stimulate Gastric acid secretion:
• Neurocrine, which releases Ach
• Endocrine, release of Gastrin from Antral G-cells
• Paracrine, release of histamine from Mast cells in the lamina propria.
• Gastric ulcers may primarly be caused by the break down of the mucosal barrier and subsequent back diffusion of acid across the Gastric mucosa.
STRESS RELATED ULCERATION
• Definition:- can be defined as superficial erosions of the gastric mucosa that develop when severe physiologic demands are placed upon a critically ill individual.
• Pathogenisis:- pathogenic mechanisms involved in the formation of stress ulcers include reduced mucosal blood flow, presence of gastric acid and disruption of mucosal barriers.
DRUG INDUCED ULCERATION
• Prolonged ingestion of NSAIDs is the major cause of GU,
• NSAIDs are thought to induce the damage of the gastric mucosa via two mechanisms
• by direct effects of the acidic agent on the gastric mucosa
• by inhibiting the production of protective prostaglandins.
ANTIULCER ACTIVITY PYLORUS LIGATION IN RATS (SHAY)
Principle:- the method allows the both qualitative assessment of ulceration and quantative assessment of acidity.
A simple and reliable method for production of gastric ulceration in the rat based on ligature of the pylorus as been published by SHAY.
The ulceration is caused by accumulation of acidic gastric juice in the stomach.
Requirements:-
animals :Albino rats ( 150-170gms)
Conditions: starvation for 48hrs
Cages with raised bottoms of wide wire mesh ( in order to avoid cannibalism and coprophagy)
Route : oral or SC
PROCEDURE
1. Rats are starved with access to drinking water.
2. Rats are housed single in cages with raised bottoms
3. Ten animals are used per dose and as controls
4. under ether anesthesia a midline abdominal incision is made. The pylorus is ligated carefully neither damaging the blood suppl, nor producing traction
5. (prepration got by application of weight)
6. The abdominal wall is closed by sutures
7. The test compound are given either orally by gavage or injected SC
8. The animals are placed for 19hrs in plastic cylinder with an inner diameter of 45mm being closed on both ends by wire mesh.
9. The animals are sacrificed in co2 anesthesia.
10. The abdomen is opened and a ligature is placed around the esophagus close to the diaphragm
11. The stomach is removed, and the contents are drained in a centrifuge tube.
12. Along the greater curvature the stomach is opened and pinned on the cork plate
13. The mucosa is examined with a stereomicroscope.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Lesions occur mainly in the lumen and in the antrum, the no of ulcers is noted and severity recorded with the following scores
0= no ulcers
1= superficial ulcers
2= deep ulcers
3= perforation
the volume of the gastric content is measured.
After centrifugation ,acidity is determined by titration with 0.1N NaOH
EVALUATION
An ulcer index UI is calculated
UI=UN+US+UPX10-1
UN=average of no of ulcers per animal
US=average of severity of score(0,1,2,3)
UP=percentage of animals with ulcers
Ulcer index and acidity of the gastric content of treated animals are compared with controls. using various doses, dose response curves can be established for ulcer formation and gastric acid secretion.
ID50 values can be caluculated by probit analysis where by 0% corresponds to no and 100% to maximal stimulated gastric acid output.
Critical assessment of the method
The “ shay-rat “ as been proven to be valuable tool to evaluate antiulcer drug with various mechanisms of action.
Stress Ulcer Through Immobilization Stress.
Principle:
Psychogenic factors such as stress, play a major role in the pathogenisis of gastric ulcers in man .
The first report of the use of restraint (device used in aiding the immobilization ) as stress factor was published by Selye.
Purpose.
study the effect of antiulcer drugs on immobilization stress in rats.
Requirements:
animals-10 female wister rats( 150-170g)
conditions-Food and water are withdrawn 24hrs before experiment.
route: oral /SC
Procedure:
1. Groups of 10 rats/dose of test drug and for control are used.
2. Food and water are withdrawn 24 hours before the expt.
3. After oral/s.c administration of the test compound or the placebo solution the animals are slightly anesthetized with ether.
4. Both lower and upper extremities are fixed together and the animals wrapped in wire gaze.
5. They are horizontally suspended in the dark at 200 for 24hours and finally sacrificed in CO2 anesthesia.
6. The stomach is removed ,fixed on a cork plate and the number and severity of ulcers is recorded with a stereomicroscope using the following scores,
0= no ulcers
1= superficial ulcers
2= deep ulcers
3= perforation
CRITICAL ASSESSMENT OF THE METHOD
The experimental model resembles the psychogenic factors in the pathogenesis of gastric ulcers in patients.therefore it is not surprising that not only antacids,anticholinergics, H2 antagonists,proton-pump nhibitors,but also psychotropic drugs,like neuroleptics,have been antagonists,proton-pump inhibitors,but also psychotropic drugs,like neuroleptics,have been found to be effective in this test.the test is being used in final drug evaluation only.
STRESS ULCERS BY COLD WATER IMMERSION
PRINCIPLE: -cooling of rats in water during the restraint period accelerates the occurrence of gastric ulcers and shortens the time of necessary immobilization
Req: -
animals:8-10 rats(150-200g)
route:oral
conditions:individual restraint cages in water
Procedure:-
Animals are taken,test compound is given orally .then placed vertically in individual restraint cages in water at 220c for one hour(in the last method restraint was used for 24 hours)
they are removed ,dried and injected intravenously via tail vein 30mg/kg evans blue.
10 min later ,they are sacrificed in CO2 anesthesia and their stomachs removed.
Formol-saline(2%v/v)is then injected into the totally ligated stomachs for overnight storage.
Next day, the stomachs are opened along the greater curvature,washed in warm water,and examined under a 3 fold magnifier.
The lengths of the longes diameters of the lesions are measured and summated to give a total lesion score(in mm) for each animal,the mean count for each group being calculated.
EVALUATION
The mean score in control rats is about 25(range20-28).inhibition of the lesion production is expressed as percentage value.
Critical assessment of the method
Like other stress models,the test resembling the psychogenic factor for ulcer disease in human beings,is used for final drug evaluation only.
INDOMETHACIN INDUCED ULCERS IN RATS
PRINCIPLE:- NSAIDs ,like Indomethacin and acetyl salicylic acid ,induce gastric lesions in man and in experimental animals by inhibition of gastric cyclo-oxygenase resulting in less formation of prostacyclin,the predominant prostanoid produced in the gastric mucosa.
Req: -
animals:8-10 rats (150-200g)
route:oral.
Procedure:
The test drugs are administered orally in 0.1% tween 80 solution.10min prior to oral Indomethacin in a dose of 20mg/kg.
6hours later,the rats are sacrificed in CO2anesthesia and their stomachs removed.
Formol-saline(2%v/v)is then injected into the totally ligated stomachs for overnight storage.
Next day, the stomachs are opened along the greater curvature,washed in warm water,and examined under a 3 fold magnifier.
The lengths of the longes diameters of the lesions are measured and summated to give a total lesion score(in mm) for each animal,the mean count for each group being calculated.
EVALUATION
The mean score in control rats is about 25(range20-28).inhibition of the lesion production is expressed as percentage value.
Modification of the method
Instead of Indomethacin,gastric lesions can be induced by intravenous or oral doses of aspirin which can be prevented by exogenous PGE2 OR PGI2.
Critical assessment of the method
Cold stress induced ulcer formation ,an be inhibited by H2 receptor antagonists have only protective effects.
CYSTEAMINE –INDUCED DUODENAL ULCERS IN RAT
Principle: -
Duodenal ulcers can be induced in rats by repeated administration of cysteamine or propionitrile in rats.
Req:-male Sprague Dawley rats(with 200g initial weight)
Procedure
Male Sprague Dawley rats are taken .
Cysteamine HCL is administered three times on day 1 in a dose of 280mg/kg orally.
Protective drugs,such as H2 antagonists ,are given 30min prior cysteamine treatment.
Rats are sacrificed on 3rd day.
For histological evaluation
The stomach and duodenum are fixed in 10% aqueous buffered formaldehyde and paraffin – embedded sections are stained with hematoxylin and eosin.
Duodenal ulcers develop in the anterior and posterior wall of the proximal duodenum, about 2-4mm from the pylorus.
The more severe ulcers, located on the anterior wall, frequently perforate, resisting in focal or generalized peritonitis or penetrate and the liver . the opposite ulcer invariably penetrates in to the pancreas.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Evaluation
The intensity of duodenal ulcers is evaluated using scores from 0-3.
0=no ulcers
1=superficial mucosal erosion
2=deep ulcer usually with transmural necrosis.
3=perforated or penetrated ulcer.
Critical assessment of the method
In view of the development of modern gastric K+/H+-ATPase Inhibitors the predictive value of methods using experimental ulcers in the rat for clinical healing rats in man has been challenged.
GASTRIC PERFUSION IN THE RAT
PRINCIPLE:-The Inhibitors of gastric acid secretion i,e antagonists act by increasing the pH from lower to higher range.
• The acid is produced due to stimulation by the histaminics, Cholinergic drugs etc.
• Thus is antagonized by drugs such as vasopressin, atropine etc. This method is for secondary screening of active agents or for comparing known agents.
Procedure:-
1. Rats are anesthetized with 25% aqueous urethane solution. Body temperatue is stabilized at 30oc
2. The trachea is cannulated
3. Polythene tube (11cms long and 2mm external diameter) is passed in to the lower esophagus .
4. The jugular veins are exposed and cannulated ; one is connected to the Manometer .
5. The abdomen is opened and the pylore duedonal junction is exposed .
6. A small glass cannula is introduced, through a cut in the duedonum, in to the stomach.
7. stomach is incised about 3cms long beginning as near as the fundus as possible.
8. Clean the stomach and wash with saline.
9. Suture the stomach and abdomen is then closed by two or three interrupted sutures.
10. The suture is then perfused continuously with a dilute solution of warm 0.00025 N NaOH which enters through the Polyethylene cannula and flows through the Glasss cannula.
11. The fluid emerging from the Pylorus passes over a glass electrode which records the pH continuosly.
12. There is found to be a linear relation between pH and acidity.
13. The rate of perfusion is about 1ml per min.after passing through the unstimulated stomach,the effluent has a pH 6.0-6.5.
14. Drugs are given through one jugular vein,in 0.1 to 0.4ml,followed by 0.1ml saline.for comparison,histamine dihydrogen phosphate is given,which cause the pH to fall from 6.0-4.0.after about 14min.carbachol is also very active.
For assay of inhibitors of gastric acid secretion,antagonists are administered intravenously immediately before,or accompanying the agonist.(e.g.histamine).
• --vasopressin is a standard inhibitor at 120-480 milli units.
• --atropine is also used as inhibitor
• Other methods used for screening.
ISOLATE RAT STOMACH
It was recommended for evaluation of H2 receptor antagonists
ISOLATED GASTRIC MUCOSAL PREPARATION
For studying the pharmacology of gastric secretion and synthesis or release of endogenous substance
PRIMARY CULTURE OF RAT GASTRIC EPITHELIAL CELLS
An in vitro model for evaluation of antisecretory agents using primary cultures of rat gastric epithelial cells.
EVALUATION OF ANTACIDS
The main activity of antacids to reduce the acidity of the gastric content thrrough neutralization and increasing The intragastric pH
Ethanol
Induced mucosal damage in rats(cytoprotective activity) ethanol produces gastric lesions in experimental animals it is inhibited by drugs, such as prostaglandins (Pg’s) have very limited relevance to prediction of ulcer healing potential in humans.
Reference
H.Gerhard Vogel,Drug Discovery and evaluation,second Edition,springer-verlag berlin Heidelberg 2002:867-873.
Bytzer P, O'Morain C: Treatment of Helicobacter pylori. Helicobacter 2005;10(Suppl 1):40.
Capell MS: Clinical presentation, diagnosis, and management of gastroesophageal reflux disease. Med Clin North Am 2005; 89:243.
Chan FK, Leung WK: Peptic-ulcer disease. Lancet 2002;360:933.
Dekel R, Morse C, Fass R: The role of proton pump inhibitors in gastro-oesophageal reflux disease. Drugs 2004;64:277.
Miner P et al: Gastric acid control with esomeprazole, lansoprazole, omeprazole, pantoprazole, and rabeprazole: A five-way crossover study. Am J Gastroenterol 2003;98:2616.
Suerbaum S, Michetti P: Helicobacter pylori infection. N Engl J Med 2002;347:1175.
1. Wolfe WM, Sachs G: Acid suppression: Optimizing therapy for gastroduodenal ulcer healing, gastroesophageal reflux disease, and stress-related erosive syndrome. Gastroenterology 2000;118(Suppl 1):S9.
1. Black, J. Reflections on the analytical pharmacology of histamine H2-receptor antagonists. Gastroenterology, 1993, 105:963–968. [PMID: 8104839]
2. Chong, E., and Ensom, M.H. Pharmacogenetics of the proton pump inhibitors: a systematic review. Pharmacotherapy, 2003, 23:460–471. [PMID: 12680476]
3. Cook, D., Guyatt, G., Marshall, J., et al. Comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N. Engl. J. Med., 1998, 338:791–797. [PMID: 9504939]
4. Dickson, E.J., and Stuart, R.C. Genetics of response to proton pump inhibitor therapy: clinical implications. Am. J.Pharmacogenomics, 2003, 3:303–315. [PMID: 14575519]
5. Fackler, W.K., Ours, T.M., Vaezi, M.F., and Richter, J.E. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology, 2002, 122:625–632. [PMID: 11874994]
6. Freston, J., Chiu, Y.L., Pan, W.J., Lukasik, N., and Taubel, J. Oral bioavailability of pantoprazole suspended in sodium bicarbonate solution. Am. J. Health Syst. Pharm., 2003, 60:1324–1329.
7. Graham, D.Y. Therapy of Helicobacter pylori: current status and issues. Gastroenterology, 2000, 118:S2–S8.
8. Howden, C.W., and Hunt, R.H. Guidelines for the management of Helicobacter pylori infection. Ad Hoc Committee on the Practice Parameters of the American College of Gastroenterology. Am. J. Gastroenterol., 1998, 93:2330–2338. [PMID: 9860388]
9. Klinkenberg-Knol, E.C., Festen, H.P., Jansen, J.B., et al. Long-term treatment with omeprazole for refractory esophagitis: efficacy and safety. Ann. Intern. Med., 1994, 121:161–167. [PMID: 8017742]
10. Kuipers, E.J., and Meuwissen, S.G. The efficacy and safety of long-term omeprazole treatment for gastroesophageal reflux disease.
11. Lanza, F.L. A guideline for the treatment and prevention of NSAID-induced ulcers. Members of the Ad Hoc Committee on Practice Parameters of the American College of Gastroenterology. Am. J. Gastroenterol., 1998, 93:2037–2046. [PMID: 9820370]
12. Richter, J.E. Gastroesophageal reflux disease during pregnancy. Gastroenterol. Clin. North Am., 2003, 32:235–261. [PMID: 12635418]
13. Rostom, A., Dube, C., Wells, G., et al. Prevention of NSAID-induced gastroduodenal ulcers. In, The Cochrane Library, Issue 2. John Wiley & Sons, Ltd., Chichester, UK, 2004.
14. Sandevik, A.K., Brenna, E., and Waldum, H.L. Review article: the pharmacological inhibition of gastric acid secretion-tolerance and rebound. Aliment. Pharmacol. Ther., 1997, 11:1013–1018.
15. Suerbaum, S., and Michetti, P. Helicobacter pylori infection. N. Engl. J. Med., 2002, 347:1175–1186. [PMID: 12374879]
16. Wolfe, M.M., and Sachs, G. Acid suppression: optimizing therapy for gastroduodenal ulcer healing, gastroesophageal reflux disease, and stress-related erosive syndrome. Gastroenterology, 2000, 118:S9–S31.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE








