


ABOUT AUTHOR
Dr. R. S. Thakur
Email: drramsthakur@gmail.com
Phone: +91-9740802164
Preamble
Health has direct impact on socio-economic growth of the country and welfare of its people. Hospital Pharmacy of a Hospital or other Health Care Facilities makes available drugs, devices, and other materials used in the diagnosis, mitigation, prevention and treatment of injury, illness, and disease. Hospital Pharmacy procures, stores and supplies medicines for dispensing, compounding, distribution and provides Pharmaceutical Care. Talking from a patient’s perspective, hospital pharmacy services provide medicines, information and advice to inpatients and outpatients as well as to the health professionals and others giving health care to the patients.
" the Pharmacist is a knowledgeable practitioner, who in cooperation with medical and nursing staff ensures the most effective, safe and economical use of drugs and rational therapy.
In the wake of advancements there are much more services rendered by hospital pharmacy, which is not visible to the patient, and these include –
1. Ensuring the appropriate purchase of medicines;
2. Quality assurance of medicines provided to the patients;
3. Establishing safe systems for storage and supply of medicines;
4. Preparation of Hospital Formularies;
5. Budgetary Planning and economic implementation;
6. Patient centered services closely linked to the Clinical team;
7. Reducing medication errors and medication related risk to patients;
8. Reducing financial risk to hospitals;
9. Organization and Functioning of Pharmacovigilance setup;
10. Education & Training to pre-registration Pharmacists;
11. Continuing education for in-service Pharmacists and other health professionals;
12. Application of Information Technology for proper management of the services;
13. Clinical Pharmacy practice & Research;
Introduction
The historical developments in the field of hospital pharmacy and modern pharmaceutical care being provided in developed world which are relevant for revamping hospital pharmacy services in India and setting up of a Directorate of Pharmacy at Central and State level are summarized and presented in this article as a guidance for modernizing and restructuring Hospital Pharmacy Service on par with developed world.
Up to 1940s majority of hospital pharmacists were engaged in traditional pharmaceutical activities relating to pounding, pouring, leaking and sticking. However, introduction of many new drugs during this period revolutionized therapy, as highly potent medicines were made available. This drastically changed the scenario and extemporaneous preparation of medicines in the Pharmacy was replaced by large scale production of medicines by industries, entailing substantial change in the role and functions of hospital pharmacists.
Section 104 of the Model State Pharmacy Act and Model Rules[1] of the National Association of Boards of Pharmacy, August 2019 defines the practice of pharmacy as follows:
“The “Practice of Pharmacy” means, but is not limited to, the interpretation, evaluation, Dispensing, and/or implementation of Medical Orders, and the initiation and provision of Pharmacist Care Services. The Practice of Pharmacy also includes continually optimizing patient safety and quality of services through effective use of emerging technologies and competency-based training.”
Historical Events
In 1951 hospital pharmacy was defined in America as a service under the direction of a pharmacist –
(i) from which all medications are supplied;
(ii) where special prescriptions are filled;
(iii) where injectables should be prepared, and
(iv) where supplies are often stocked.
In 1955 the Linstead report on the hospital pharmaceutical services underlined the role of hospital pharmacist as under-
(i) dispensing of drugs
(ii) promoting economy in usage of drugs, and
(iii) instructing or advising those who handle the services provided
The 1960s emerged as the starting point for development of “Ward Pharmacy” emanating from growing awareness of high incidence of medication errors at ward levels. [2] This led to development of more advanced prescription charts and the need to keep these on the wards. The functions of ward pharmacy include drug supply, stock control, prescription monitoring and drug information for doctors, nurses and patients. This was felt more necessary due to introduction of wide range of new potent medicines in clinical practice which posed potential risks and increased Adverse Drug Reactions (ADRs). Further revamping of Hospital Pharmacy (HP) services became inevitable with introduction of new dosage forms and novel drug delivery systems.
The realization for specialization within hospital pharmacy was recognized in 1965 and quality assurance was introduced as one of the key role and responsibility of hospital pharmacy.
In the late 1960s the concept of “clinical pharmacy” began sprouting to further reorient the practice of pharmacy towards patients and involvement of Pharmacists in drug usage. [3] This was transition of the role of Pharmacist from product oriented to patient oriented where his deep knowledge and expertise in pharmaceutics, pharmacology, toxicology, pharmacokinetics, analysis and therapeutics is directly utilized to individualize the medication to be used. This service includes but is not limited to patient interviews on drug therapy, participation in patient care rounds, Adverse Drug Reaction reporting, Therapeutic drug monitoring, answering drug information queries, and patient counselling on discharge.
In 1970, drug information became another specialty service of the Hospital Pharmacy. This is one area where information technology is extensively used to provide prompt and accurately evaluated information to all health care providers.
Hathi Committee Recommendations (1975)
Report of the Committee on Drug and Pharmaceutical industry (April, 1975) popularly known as Hathi Committee report [4] observed that hospital pharmacy services contribute a great deal to the overall quality of medical services rendered by hospitals. The report appreciated the step taken by Union Deputy Minister for Health and Family Planning vide his D. O. letter No. F.3-13/70-D dated 17th June, 1971 to Health Minister of all States and Union Territories for improvement of hospital pharmacy to ensure that patients in hospitals receive drugs of quality. The report endorsed the recommendations of the meeting of Drug Standard Control Officers from the Centre and the States. The recommendations are quoted hereunder:-
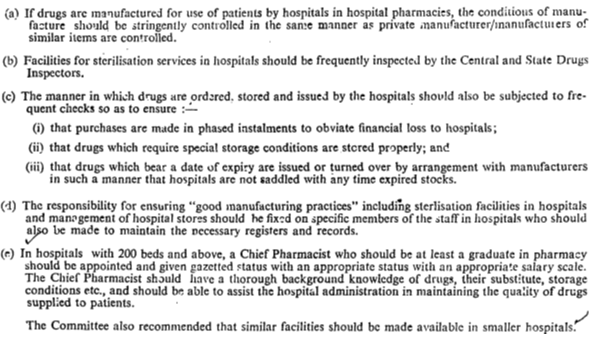
The report discussed detailed procedure for functioning of Hospital Pharmacy in not fewer than 11 heads running through page 240 to 244. These are still gathering dust in the corridors of power and the hospital pharmacy services remain in out dated shape.
In 1980, the English Regional Pharmaceutical officers developed the standards for the Hospital Pharmacy services which was revised in 1989 and all together contain 28 areas of Pharmaceutical care/ practice including –
(i) Purchase of drugs & appliances
(ii) Supply of medicines
(iii) Stock management
(iv) Clinical pharmacy services
(v) Drug information services,
(vi) Technical services
(vii) Repacking/ pre-packing assembly
(viii) Non-sterile manufacturing
(ix) Sterile manufacturing
(x) Aseptic preparations
(xi) Education & training for hospital technical services
(xii) Quality assurance of medicines and devises
(xiii) Clinical Research & Developoment
(xiv) Drug Therapy Management
(xv) Drug regimen review
(xvi) Advisory services
(xvii) Serving on Various hospital committees
(a) Pharmacy & Therapeutics Committee
(b) Hospital Infection Control Committee
(c) Human ethics committee
(d) Animal ethics committee
(e) Institutional Review Board
(f) Clinical trial committee
(xviii) Clinical governance and risk management
(xix) Ward pharmacy
(xx) ADR monitoring & reporting
(xxi) Patient counselling
(xxii) Hospital pharmacy management
(a) Staff management
(b) Budget management
(c) Benchmarking
(xxiii) Application of information technology
(xxiv) Maintenance of patient record
(xxv) Clinical specialty linked services
(xxvi) Specialist information services
(xxvii) Health education and
(xxviii) Hospital Formulary Services.
Some of the functions of hospital Pharmacists are discussed to explore the importance of these services and need for modernization to provide world class health care.
“Pharmaceutical Care” is that provision of Drug therapy and other patient care services which intends to achieve outcomes related to the cure or prevention of a disease, elimination or reduction of a patient’s symptoms, or arresting or slowing of a disease process. Pharmaceutical Care encompasses the process through which Pharmacists, in cooperation with the patient and other professionals, design, implement, and monitor a therapeutic plan for the purpose of improving a patient’s quality of life. [5,6] Objectives of Pharmaceutical Care include cure of a disease, elimination or reduction of a patient’s symptoms, arresting or slowing of a disease process, or prevention of a disease or symptoms. The process includes three primary functions:
(1) identifying potential and actual Drug-related problems;
(2) resolving actual Drug-related problems; and
(3) preventing potential Drug-related problems.
Pharmaceutical Care needs to be provided by all Pharmacists to the extent of their abilities in greater interest of the patient.
“Drug Regimen Review” covers the following activities by the pharmacist:
(1) Evaluation of the Prescription Drug Order(s) and patient record(s) for:
(i) known allergies;
(ii) rational therapy-contraindications;
(iii) reasonable dose and route of administration; and
(iv) reasonable directions for use.
(2) Evaluation of the Prescription Drug Order(s) and patient record(s) for duplication of therapy.
(3) Evaluation of the Prescription Drug Order(s) and patient record(s) for interactions:
(i) Drug-Drug interactions;
(ii) Drug-food interactions;
(iii) Drug-disease contraindications; and
(iv) Adverse Drug reactions.
(4) Evaluation of the Prescription Drug Order(s) and patient record(s) for proper utilization (including over- or under-utilization), and optimum therapeutic outcomes.
“Medication Therapy Management” aims at review of Drug therapy regimen(s) of patients by one or more Pharmacists for the purpose of evaluating and rendering advice to one or more Practitioners regarding adjustment of the dosage regimen. Decisions involving Medication Therapy Management is made in the best interest of the patient. Medication Therapy Management offers overall cost reduction and better outcomes of therapy. [7] This specialty practice includes:
(1) Implementing, modifying, and managing Drug therapy;
(2) Collecting and reviewing patient histories;
(3) Obtaining and checking vital signs, including pulse, temperature, blood pressure, and respiration;
(4) Ordering and evaluating the results of laboratory tests directly related to drug therapy; and
(5) Such other patient care services as required for best clinical outcomes and allowed by law.
“Patient Counselling” is oral communication of information by the Pharmacist, to the patient or caregiver, in order to ensure proper use of drugs and devices, so as to encourage patient compliance.
In October 1983, Nuffield foundation (UK) appointed a committee [8] under the Chairmanship of Sir Kenneth Clucas, former Permanent Secretary, Department of Trade “to consider the present and future structure of the practice of pharmacy in its several branches and its potential contribution to health care and to review the education and training of pharmacists accordingly”.
Summary of the Committee’s report is reproduced below:
“The most significant development in hospital pharmacy and possibly the most interesting activities within the profession has been the introduction of clinical pharmacy, [9-12] this has owed much to the initiative, dedication and enthusiasm of individuals, both pharmacists and doctors. For the most part this has been done without additional resources through the expedient of automating what can be automated and delegating what can be delegated, thus releasing professional resources for professional work. Attempts to assess benefits of this work against its costs have proved difficult. We think clinical pharmacy looks so promising as to warrant its extension to all hospitals.
Another significant development has been the acceptance of the principle of specialization both between different areas of pharmacy and between different medical areas within clinical pharmacy. We consider this process both inevitable and desirable.
One desirable consequence of the development of clinical pharmacy is the increasing cooperation to which it has led between the health care professions. The principal beneficiary of this is the patient. There is a scope for increasing the pharmacist’s contribution to inter-professional cooperation in such areas as ADRs reporting and clinical trials.”
Functions of Hospital Pharmacy Services:
Procurement: Drug Selection, Purchasing, Responsibility, and Control - The selection of pharmaceuticals is a basic and extremely important professional function of the hospital pharmacist who is charged with making decisions regarding products, quantities, product specifications, and sources of supply. It is the pharmacist’s obligation to establish and maintain standards assuring the quality, proper storage, control, and safe use of all pharmaceuticals and related supplies (e.g., fluid administration sets); this responsibility must not be delegated to another individual. The setting of quality standards and specifications requires professional knowledge and judgment and must be performed only by the pharmacist. Economic and therapeutic considerations make it necessary for hospitals to have a well controlled, continuously updated formulary. It is the pharmacist’s responsibility to develop and maintain adequate product specifications to aid in the purchase of drugs and related supplies under the formulary system. The IP/ BP/ USP/ NF are good source for drug product specifications. There should be standard criteria to evaluate the acceptability of manufacturers and distributors. In establishing the formulary, the Pharmacy & Therapeutic committee recommends guidelines for drug selection. Although the pharmacist has the authority to select a brand or source of supply, he must make economic considerations subordinate to those of quality. Competitive bid purchasing is an important method for achieving a proper balance between quality and cost when two or more acceptable suppliers market a particular product meeting the pharmacist’s specifications. In selecting a vendor, the pharmacist must consider price, terms, shipping times, dependability, quality of service, returned goods policy, and packaging. Moreover, prime importance always must be placed on drug quality and the manufacturer’s reputation. It should be noted that the pharmacist is responsible for the quality of all drugs dispensed by the pharmacy.
Records. The pharmacist must establish and maintain adequate recordkeeping systems. Various records must be retained (and be retrievable) by the pharmacy because of governmental regulations; some are advisable for legal protection, others are needed for accreditation, and still others are necessary for sound management (evaluation of productivity, workloads, and expenses and assessment of departmental growth and progress) of the pharmacy department. Records must be retained for at least the length of time prescribed by law (where such requirements apply). It is important that the pharmacist study central, state, and local laws to become familiar with their requirements for permits, tax, storage of alcohol and controlled substances, records, and reports. Among the records needed in the drug distribution and control system are
Receiving Drugs.
Receiving supplies should be under the auspices of a responsible individual, and the pharmacist must ensure that records and forms provide proper control upon receipt of drugs. Complete accountability from purchase order initiation to drug administration must be laid down. Person involved in the purchase, receipt, and control of drugs should be well trained in their responsibilities and duties and must understand the serious nature of drug. All nonprofessional personnel employed by the pharmacy should be selected and supervised by the pharmacist. Delivery of drugs directly to the pharmacy or other pharmacy receiving area is highly desirable; it should be considered mandatory for controlled drugs. Orders for controlled substances must be checked against the official order blank (when applicable) and against hospital purchase order forms. All drugs should be placed into stock promptly upon receipt, and controlled substances must be directly transferred to safe and secure areas.
Drug Storage and Inventory Control.
Storage is an important aspect of the total system. Proper environmental control (i.e., proper temperature, light, humidity, conditions of sanitation, ventilation, and segregation) must be maintained wherever drugs and supplies are stored. Storage areas must be secure; fixtures and equipment used to store drugs should be constructed so that drugs are accessible only to designated and authorized persons. Such persons must be carefully selected and supervised. Safety is another important factor, and proper consideration should be given to the safe storage of poisons and flammable compounds. Medicines for external use should be stored separately from internal medications. Medications stored in a refrigerator containing items other than drugs should be kept in a secured separate compartment. Proper control is important wherever medications are kept, whether in general storage in the institution or the pharmacy or patient-care areas (including satellite pharmacies, nursing units, clinics, emergency rooms, operating rooms, recovery rooms, and treatment rooms). Expiration dates of perishable drugs must be considered in all of these locations, and stock must be rotated as required. A method to detect and properly dispose of out dated, deteriorated, recalled, or obsolete drugs and supplies should be established. This should include monthly audits of all medication storage areas in the institution. The results of these audits should be documented. Since the pharmacist must justify and account for the expenditure of pharmacy funds, he must maintain an adequate inventory management system. Such a system should enable the pharmacist to analyze and interpret prescribing trends and their economic impacts and appropriately minimize inventory levels. It is essential that a system to indicate subminimum inventory levels be developed to avoid shortages, along with procedures to procure emergency supplies of drugs when necessary.
In-House Manufacturing, Bulk Compounding, Packaging, and Labelling. As with commercially procured drug products, those produced by the pharmacy must be accurate in identity, strength, purity, and quality. Therefore, there must be adequate process and finished product controls for all manufacturing/bulk compounding and packaging operations. Written master formulas and batch records including product test results must be maintained. All technical personnel must be adequately trained and supervised. Packaging and labelling operations must be adequately controlled to prevent product/package/label mix-ups. A lot number to identify each finished product with its production and control history must be assigned to each batch following the labelling requirements of Drugs and Cosmetics Rules.
The Good Manufacturing Practices is a useful model for developing a comprehensive control system. The pharmacist prepares those drug dosage forms, strengths, and packaging that are needed for optimal drug therapy but commercially unavailable. Adequate attention must be given to the stability, palatability, packaging, and labelling requirements of these products.
Medication Distribution (Unit Dose System).
Medication distribution is the responsibility of the pharmacy. The pharmacist, with the assistance of the Pharmacy & Therapeutics committee, must develop comprehensive policies and procedures that provide for the safe distribution of all medications and related supplies to inpatients and outpatients. For reasons of safety and economy, the preferred method to distribute drugs in institutions is the unit dose system. Although the unit dose system may differ in form depending on the specific needs, resources, and characteristics of each hospital. Five elements are common to all:
(1) medications are contained in, and administered from, single unit or unit dose packages;
(2) medications are dispensed in ready-to-administer form to the extent possible;
(3) for most medications, not more than a 24-hour supply of doses is provided to or available at the patient-care area in the hospital ward at any time;
(4) a patient medication profile is concurrently maintained in the pharmacy for each patient; and
(5) Floor stocks of drugs are minimized and limited to drugs for emergency use and routinely used safe items such as mouthwash and antiseptic solutions.
Discussion
It is regretted that in spite of such rapid and radical development in the field of hospital pharmacy, availability of modern medicines and novel drug delivery systems for therapy, the reorganization and revamping of hospital pharmacy services remain completely neglected in India and the pattern of practice is not at all comparable to the services provided in Western World from where the modern allopathic medicine system was imported into India by British rulers. The present status of hospital Pharmacy in India is absolutely unsatisfactory as a result of which patients are unable to harness fullest benefits of modern medicines. The time since, India attained independence there have been rapid advances both in introduction of large number of highly potent new drugs and varieties of complex formulations & newer dosage forms, but unfortunately there has been no effort to modernize hospital Pharmacy Services, which is actually soul of modern therapy. Knowledge of adverse drug reactions and drug-drug, drug-food and drug-drink interactions have been enriched but their clinical benefits could not be fully utilized for lack of practice set up. Understanding of these intricacies on molecular and cellular level as well as devastating side effects and untoward effects of modern medicines are the background of emergence of Clinical Pharmacy practice in Western world in late 1960s to make medication safe, effective and economic. [13] With the introduction of every new drug or the dosage form, therapy is becoming exceedingly complex and medicines are becoming menace in absence of Pharmaceutical Care. Modern medicines are posing unimaginable health hazard if adequate and extensive precautions are overlooked either for lack of knowledge/information or negligence and public health hazards emerge. It is in this perspective that horizon of hospital pharmacy has been expanding like anything to keep pace with advances in drug delivery systems and the efficacy, safety and economic aspects of therapy (Pharmacotherapy, Pharmacovigilance and Pharmacoeconomics). Hospital Pharmacy is the hub of pharmacy practice around which the pharmaceutical services are provided.
Thus, in a nutshell, the Hospital Pharmacy Services is important in ensuring that medicines are available and used safely and effectively by informed patients and professionals, both within the hospital and by ambulatory patients. More emphasis is now given on Clinical Pharmacy practice in all hospitals and drug information services to ensure that patients avail most of the benefits of modern medicines and they are not exposed to the risk or adverse effects. Thus, patient safety and economic aspects are major concern where medicine management is not done properly.
In light of such wide gamut of services that are to be provided by Pharmacists, the Pharmacist is a knowledgeable practitioner, who in cooperation with medical and nursing staff ensures the most effective, safe and economical use of drugs and rational therapy.
CONCLUSION
Pharmacists of India can reshape their practice arena and emerge as resourceful health care professional in the eyes of the society, if Directorate of Pharmacy is set up with the objective to modernize Pharmacy services in the country. Hospital Pharmacies must get adequate and appropriate infrastructure and support to provide world class Pharmaceutical Care. This will ensure rational drug therapy and save mankind from ill effects of medicines. It must be emphasized that without restructuring Health Care System and setting up of Directorate of Pharmacy in all States and at Centre, modernization of Pharmacy services shall remain a dream only and medication errors shall continue to play havoc on life and health of people. Sooner the Government pays attention to this dire need of modern Pharmacy Services, is better for health care achievements and health of nation. Modern medicines are two edged weapon, which is tuned by pharmacist to cure.
REFERENCES
1. Model State Pharmacy Act and Model Rules of the National Association of Boards of Pharmacy, August 2019: http://www.nabp.net; August 2008; Accessed: March 29, 2020.
2. Department of Health and Social Security, Scottish Home and Health Department, Welsh Office. Report of the Working Party on the Hospital Pharmaceutical Service (Chair: Sir N Hall). London: HMSO, 1970.
3. Statement on Clinical Pharmacy. Leicester: United Kingdom Clinical Pharmacy Association, 1983.
4. Report of the Committee on Drug and Pharmaceutical industry (April, 1975) Hathi Committee report. P 240-244.
5. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990; 47:533-43.
6. Lobas NH, Lepinski PW, Abramowitz PW. Effects of pharmaceutical care on medication cost and quality of patient care in an ambulatory-care clinic. Am J Hosp Pharm. 1992; 49:1681-8.
7. The Lewin Group. Medication therapy management services: a critical review. J Am Pharm Assoc. 2005; 45:580- 587. https://www.ncbi.nlm.nih.gov/pubmed/16295643 Accessed: March 29, 2020.
8. Pharmacy. The Report of a Committee of Inquiry appointed by the Nuffield Foundation (Chair: Sir K Clucas). London: The Nuffield Foundation, 1986.
9. Harrison P1, Standing VF and Watling JJ. Clinical Pharmacy. A statement from the Regional Pharmaceutical Officers' Committee. 1988.
10. Department of Health, Health Services Management. The Way Forward For Hospital Pharmaceutical Services. HC(88)54. London: UMSO, 1988.
11. Department of Health. Health Services Management. The way forward for hospital pharmaceutical services. 1988(GEN)32. Edinburgh: HMSO, 1988.
12. Department of Health and Social Services. Health Services Management. The way forward for hospital pharmaceutical services. 1989(GHS)2. Belfast: HMSO, 1989.
13. Smith WE. The future role of the hospital pharmacist in the patient care area. Am J Hosp Pharm. 1967; 24:228-31.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT admin@pharmatutor.org
FIND OUT MORE ARTICLES AT OUR DATABASE






