About Authors
About Authors
Mr. Suman Saha1*, Dr. S.Chakraborty2, Dr. A.K.Bandyopadyay3
1 M.Pharm, Dept. of Pharmaceutical Technology, Jadavpur University, Kolkata
2 MD, Consultant Anaesthesiologist, AMRI hospitals, Kolkata
3 Professor, Dept. of Pharmaceutical Technology, Jadavpur University, Kolkata
*suman.ju01@gmail.com
Abstract:
Pain is the most common symptom prompting patients to seek medical attention and is reported by more than 80% of individuals who undergone their preliminary treatment. In case of surgery most of the patients suffer from mild to severe pain due to huge number of tissue damage. Thus pain control is an important part for the patients who had undergone some surgery. Good pain control is needed to prevent the negative outcomes such as tachycardia, hypertension, Myocardial Ischemia etc. and provide better medical outcome. Pain can be assessed by different techniques but the most widely accepted technique is Visual analog scale (VAS) method. This article reviews a number of paper published internationally over this emergent topic and gives a brief overview related to pain assessment technique, mechanism of pain management and newer approaches taken to control pain.
[adsense:336x280:8701650588]
REFERENCE ID: PHARMATUTOR-ART-1725
Introduction:
According to the “International Association for the Study of Pain”, Pain is ‘An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage’.1
Proper control of Post-Operative pain plays an important role in perioperative pain management. Taking the fact that, beyond the fear for outcome of a surgery, the main concern of patients is post-operative pain’s intensity. Post-Operative pain occurs due to tissue damage caused by the surgical procedures and it is the expression of autonomic responses which can produce unwanted sensory or emotional experiences.2
Over the past decade, medical societies, governmental agencies, and Joint Commission on Accreditation of Healthcare Organizations (JCAHO) have increased their attention to manage the Post-Operative pain intensity.3
In USA, survey of 250 patients who had undergone surgery in the last 5 years before 2008 revealed that 82% reported Post-Operative pain and 86% reported that the pain intensity is moderate, severe or extreme pain.3
Good pain control is needed to prevent negative outcomes such as Tachycardia, Hypertension, Myocardial Ischemia, decrease in alveolar ventilation and poor wound healing. Aggravation of pain can lead to neural sensitization and release of mediators both peripherally or centrally.4
Post surgical pain mechanism:
[adsense:468x15:2204050025]
Tissue injury caused by surgery has two essential factors. An inflammatory and a neuropathic component. In both cases, the pain is characterized by a increased sensitivity and response to noxious or non-noxious stimuli resulting an experience of pain.10
During surgery there are damages to the tissues, which produces noxious stimuli and nociceptive input. And in the post operative period there is inflammatory process at the injury site, which is also responsible for noxious input. Both these processes sensitize the pain pathways. They occur at peripheral level where there is a decrease in threshold of nocioceptive afferents and at a central level with an increase in excitation of spinal neurons involved in pain transmission. This noxious stimuli is resulting in tissue damage and inflammation. This leads to release of inflammatory mediators such as K, serotonin, bradykinin, Substance P, histamine etc. These substances act to sensitize high threshold nociceptors. The low threshold stimuli, which could not normally cause pain, are now feels painful. 5
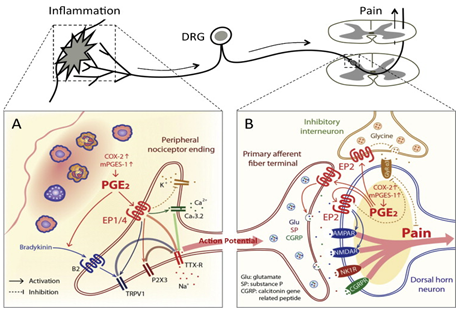
Inflammatory pain mechanism (Fig-1)
Neuropathic pain is the other element in tissue injury occurred in surgical procedures. This is induced by damage to the nerves traversing the surgical site. As a consequence of such lesion to the peripheral nervous system, there might be some sensory, motor or autonomic changes. In practice it is the damage to afferent sensory nerves that is responsible for the neuropathic pain part. When lessions occur, they may cause sensory loss in the innervation territory corresponding to the damaged nerves or the peripheral projections of central nervous system structures. So, an important distinguishing feature in several neuropathic types of pain is the paradoxical combination of sensory loss and pain with or without sensory hypersensitivity phenomenon in the painful area.11
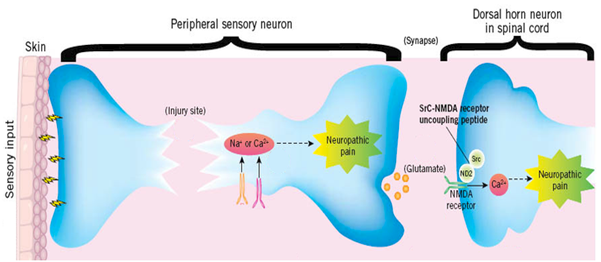
Neuropathic pain mechanism (Fig-2)
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Drugs used in Post-Operative pain managenent:
Main class of drugs that are used in post operative pain management are Opioid analgesics. Analgesics are defined as, the drugs which relieves pain without blocking nerve impulse conduction or markedly altering sensory functions. Based on the type of relieving action, analgesics are classified into two groups. Opioids inhibits pain perception by acting on bain receptors. They can be used for short term or long-term relief of pain, mainly but bears a risk of drug addiction. Opioid receptors are present in different locations. Opioids receptors are present in the periphery, Spinal cord and central nervous system. Opioids cross the blood brain barrier for its activity. Opioid have greater lipid solubility.
|
Pathophysiology of Neuropathic pain9 1. Peripheral Nerve 2. Dorsal root ganglion: 3. Spinal Nerve Root: 4. Central Nervous System (CNS): Disinhibition: Plasticity: Altered Connectivity Rostral Effects Altered physiology at rostral level. Which is caused due to caudal lesions. |
Partition coefficient determines the distribution, onset and duration of action of the drug. respiratory depression, bowel dysmotility, urinary retention, and pruritus are the major side effects. Fentanyl is an example of a lipid-soluble drug with a high potency and a rapid onset of action.12
Morphine is the model opioid with which all other analgesic drugs are compared. Intravenously use of Morphine is a better choice in the perioperative period. Intravenous morphine has an onset of action at approximately 5 minutes, a peak effect within 20 minutes, and duration of action of 3 to 4 hours. Unfortunately, morphine has a relatively high incidence of associated nausea and vomiting.13,14
Pethidine is another opiate available for perioperative use. Pethedine has a similar time-to-onset but only one tenth of the potency of morphine. In addition, it has atropine-like side effects, including tachycardia and ampullary dilatation.
Tramadol is a relatively new analgesic drug. Both tramadol and Pethidine have a similar efficacy. Tramadol may be given in doses of 50 to 100 mg orally every 4 to 6 hours in adult patients.15
Non opioids, used for short term relief of pain. They act by inhibiting synthesis of prostaglandins which are the molecules involved in the peripheral perception of pain.
NSAIDs and adjuvant analgesics are widely used for post operative pain management. Adjuvant analgesics are the drugs which have a primary indication other than pain that have analgesic properties in painful conditions. The group includes a number of drugs in different classes, such as the tricyclic antidepressants, anticonvulsants, N-methyl-D-aspartic acid receptor antagonists, low-dose intravenous local anesthetics etc. these agents are administered in cases of refractory pain. For some chronic pain syndromes, they constitute a first-line approach. Paracetamol also used to treat post operative pain management. Paracetamol may be given in doses of 1gm. three to four times a day.
N-methyl-D-aspartate receptor antagonists:
The NMDA receptor is an excitatory amino acid receptor which has been implicated in the modulation of prolonged pain states. Nociceptive stimuli increases the release of various substances including excitatory amino acids, which activate the NMDA receptors and result in their hyperexcitability. This creates a state of wind-up that leads to hyperactivity of the nociceptive system and increases the magnitude and duration of neurogenic responses to pain. Thus antagonize the action of receptor decrease the pain perception.20
Ketamine:
Ketamine is an intravenous (IV) anaesthetic with analgesic property to its action on the NMDA receptor. Several trials are investigating the use of low-dose ketamine for management of postoperative pain syndrome.
There are also new therapeutic target with analgesic properties such as: Cannabinoid receptors, Neuronal nicotinic receptors, Glutamate receptors, Calcium channel neural type N.4
Non pharmocological methods:
Though pharmacotherapy forms is an essential part of management of acute pain, there are various other methods which give relief post operative pain. The non pharmacological methods can be used as adjuvants to the main method of pain relief. Herbal medicine, Hypnosis, Homeopathy, Meditation, Trans cutaneous nerve stimulation (TENS), Acupuncture, Heat application are used as an adjuvant method to suppress pain perception.19
Herbal medicine:
Many pain medications are derived from plant extractions and are purified alkaloids. Extract from chlli pepper (capsicum) is significantly used to treat post operative pain. The active ingredient capsaician which depletes substance P from the nerve terminals and is beneficial in amputation phantom limb pain and post mastectomy surgery.16
Homeopathy:
Symptom is considered as a positive sign throwing offthe disease state. In allergyand asthma it has proven its efficacy, but not so effective in acute pain. Argumentagainst is that the method employed was noteffective.18
Hypnosis:
Is this technique mind creates focused attention.It is a self hypnosis procedure where therapist functions is to guide andhelp patient to focus attention and filter out unpleasant and negative sensation and receive positive sensation. Current research shows that it is not a passive withdrawl ofawareness but rather an active suppression of somatosensory cortex by frontal cortex.16 Anecdotal reports aboundbut growing scientific literature on the role of suggestionin preparing for surgery there by reducing the post operative pain.17
Pain assessment technique:
Assessment of pain depends on level of consciousness and degree of cooperation of the patient. In patients who are conscious and able to communicate, pain are best assessed by the help of a good history and physical examination.The two most common methods are the visual analog scale (VAS) method and the numeric rating scale (NRS) method.
The VAS consists of a straight line with the words ‘‘no pain’’ written on one end and the words ‘‘worst pain’’ written at the other end. Patients have to indicate their level of pain by placing a mark along the scale. Measurement improves when a standard 10 cm line is used. The Visual analog scale (VAS) is the most useful method as it tracks the changing pattern of a patient’s pain.
Numeric range scalethat allow client to rate pain intensity on a numbered scale, such as the 0 to 10 Numeric Pain Intensity Scale: there are also related scales which can assess pain and the degree of distress to the patient caused by the pain.21
New Approaches to treat post operative Pain:
Improvement of knowledge of molecular mechanisms had helped to development of multimodal analgesia technique and new pharmaceutical products to treat postoperative pain. The new pharmacological products to treat postoperative pain include extended-release epidural morphine and analgesic adjuvants such as capsaicin, ketamine, gabapentin, pregabalin, dexmetomidine. Newer technique that is patient-controlled analgesia (PCA) in modes such as intranasal, regional, transdermal, and pulmonary presents another interesting aspect of development to control the pain intensity.6,7,8
Discussion:
Pain has been found to be one of the most common medical causes of delayed discharge after surgery, the other two are drowsiness and nausea/vomiting. Thus a number of measures like drugs and some non pharmacological method also used to control post operative pain. Now multimodal analgesia takes a major role in post operative pain management. Despite this overwhelming rationale approach for effective postoperative pain control, the clinical reality is, unfortunately, still far from satisfactory.
References
1. International association for the study of pain, subcommittee on taxonomy, classification of chronic pain: description of chronic pain syndromes and definitions of pain term.Pain 1986: (Suppl 3):S1-225
2. Georgiana-Diana varzaru, Prof. Dr. florica Popescu: Analgesia an important element in the post operative management of the patient. Multimodal analgesia as an additional antinociceptive method. Craiova 2011
3. Mohammad Abdullah Al masud, Syed. Ashrafuzzaman and Md. Jalaluddin Iqbal: Pattern of use of analgesics in a surgical unit, 2009, Bangladesh J Pharmacol 21-23. ISSN: 1991-0088 (Online), 1991-007X (Print)
4. Nalini Vadivelu, Sukanya Mitra, deepak Narayan: Recent advancement in Post-Operative pain management; March 2010, Yale J Biol Med. 83 (1):11-25.
5. Dr.Manimala Rao: Acute Post Operative Pain; 2006, Indian J. Anaesth. 50 (5): 340-344
6. Breivik H. Postoperative pain management: why is it difficult to show that it improves outcome? Eur J Anaesthesiol. 1998;15(6):748–751.
7. Carr D, Goudas L. Acute pain. Lancet. 1999;353(9169):2051–2058.
8. Breivik H, Stubhaug A. Management of acute postoperative pain: Still a long way to go! Pain. 2008;137(2): 233–234.
9. John Scadding: Neuropathic Pain; 2003, ACNR • VOLUME 3 NUMBER 2
10. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet 2006;367:1618-25.
11. Birgitte Brandsborg: Pain following hysterectomy: Epidemiological and clinical aspects. Dan Med J 2012;59(1): B4374
12. Mitchell Jay Cohen, MD,William P. Schecter, MD, FACS:Perioperative Pain Control: A Strategy for Management; Surg Clin N Am 85 (2005) 1243–1257
13. Claxton AR, et al. Evaluation of morphine versus fentanyl for postoperative analgesia after ambulatory surgical procedures. Anesth Analg 1997;84(3):509–14.
14. Schecter WP, et al. Pain control in outpatient surgery. J Am Coll Surg 2002; 195(1): 95–104.
15. Schecter WP, Swisher JL. Local anesthesia in surgical practice. Curr Probl Surg 2000;37(1):10–67..
16. Spiegel D, Barabasz A: Effects of hypnotic instructions of P300 event related pote ntial amplitudes: research and clinical applications. Am J Clin Hypn 1988; 31 (1): 11-17.
17. Enqvist B, von Konow L, Bystedt T. Pre and perioperative suggestion in maxillofacial surgery: effects on blood loss and recovery. Int J Clin Exp Hypn 1995; 43: 284-294.
18. Whitmarsh T. Evidence in complementary and alternative therapies: lessons from clinical trials of homeopathy in headache. Jaltern Complement Med 1997; 3: 307-310.
19. Dr. Manimala Rao: Acute post operative pain; Indian J. Anaesth. 2006 ; 50 (5):340-344
20. Ashraf S. Habib, MBBCh, MSc, FRCA, Tong J. Gan, MB, FRCA:Role of analgersic adjuncts in post operative pain management; Anesthesiology Clin N Am 23 (2005) 85– 107
21. Shailaja S. Jaywant , Anuradha V. Pai: A comparative study of pain measurement scales in acute burn patient; The Indian Journal of Occupational Therapy : Vol. XXXV : No. 3
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE