About Authors:
About Authors:
*Anton Vinoth.T , Prof .K. Nagarajan , Mr. Manikandan
Department of Pharmacy practice, K.M College of Pharmacy,
Madurai, Tamilnadu
*vinoth.anton@gmail.com
ABSTRACT:
Mood disorders (affective disorders) are among the most common mental disorders encountered in clinical practice and divided into bipolar disorders and depressive disorders. The essential feature of these disorders is a major disturbance in mood. Depression is common, affecting about 121 million people world wide. At its worst depression can lead to suicide, a tragic fatality associated with the loss of about 85000 lives every year. By the year 2020, depression is projected to reach the second Major depression is among the most common mental disorders encountered in clinical practice. The problems associated with depression can become chronic or recurrent and lead to substantial impairment in an individual’s ability to take care of his or her everyday responsibilities. At its worst depression can lead to suicide, a tragic fatality associated with the loss of a large number of lives every year. Depression is the leading cause of disability as measured by YLDs and the leading contributor to the global burden of diseases (DALYs) in 2000.
The present study is done as it is the role of a clinical pharmacist to evaluate the efficacy and safety of the drugs acting through specific antidepressant mechanisms and to assess the possibility of matching patient symptom profile with antidepressant mechanism to achieve more rapid response or greater efficacy.
The aim of the study is tocompare the efficacy of Citalopram and Escitalopram in the Major Depressive Disorder Patients during the first 8 weeks (acute phase) of treatment.
[adsense:336x280:8701650588]
Reference Id: PHARMATUTOR-ART-1449
Introduction:
The term depression is reserved in psychiatry to describe a specific entity having biologic and pharmacologic implications. Studies show that the physical and social dysfunctions produced by depression outweigh most chronic medical conditions. The medical outcomes study demonstrated that the degree of impairment in depressed patients is comparable only to patients with chronic heart disease. In turn, the cost of care for depression produces a tremendous burden upon society. If co-morbid with a medical condition, and may even shorten life expectancy.
Because of high prevalence and chronicity of depression, a complete antidepressant response remains an objective for clinicians and is still a key target for new drug developments. Approximately eight classes of antidepressants acting by different mechanisms are available for the physicians for treatment.
Despite the similarity of escitalopram and Citalopram, preclinical as well as various clinical studies (including double-blinded studies) have shown differentiated effects of Citalopram and escitalopram, as well as a clinical superiority compared with a variety of other SSRIs, such as paroxetine especially in severely depressed patients A head-to-head comparison of escitalopram with duloxetine (Cymbalta) found escitalopram to be both more tolerable and more effective. Compared with venlafaxine and sertraline, escitalopram was shown to have similar efficacy.
[adsense:468x15:2204050025]
METHODOLOGY
STUDY DESIGN:
· A prospective randomized interventional study is carried out Comparative study of Citalopram and Escitalopram in the Major Depressive Disorder patients
· This is an 8 week study. Participated patients shall be visiting the hospital for periodical review, for every 2 weeks.
· This study is conduct over a period of six months including the interpretation and analysis of results.
· Totally 20 patients are selected for each groups randomly and enroll for this study.
· The result will calculate with regular follow up to analyse the efficacy and safety of Citalopram and escitalopram in major depressive disorder patient.
· The result will calculate with the help of statistics, tables and graphs.
The study was conducted in 6 phases.
Phase 1
· Discussion about the use of various types of antidepressants with the psychiatrists of M.S Chellamuthu Trust & Research Foundation Madurai.
· Enquiring of the relevance of this study with Dr.Ganesh Kumar M.B, B.S, DPM (Psychiatry), Consultant psychiatrist of M.S Chellamuthu Trust & Research Foundation Madurai.
· Collection of literatures.
Phase 2
· Designing of the methodology of the study was done.
· Case report forms were prepared and the different rating scales of depression were collected.
Phase 3
SELECTION OF SAMPLE
40 consecutive patients attending the psychiatric clinic during the study period were independently evaluated by the psychiatrist who initially did the clinical interview and arrived at a diagnosis using the ICD-10 criteria for research.
INCLUSION CRITERIA:
• Outpatients.
• Patients who met DSM-IV criteria for major depressive disorder (MDD), a single major depressive episode or recurrent major depressive episode without psychotic features, MDD are primary mental disorder.
• Age from 18-75 Years old, male or female.
• HAMD-17 total score at least 20 at baseline and first item’s score at least 2
• MADRS score greater than or equal to 22 at baseline.
• CGI-S at least 4 at baseline
• Written informed consent provided by patient himself/herself.
EXCLUSION CRITERIA:
· Severe suicide attempt.
· Any unstable medical illness would affect study or increase patient’s risk to participate this study, including disease of heart, lung, liver, kidney, cardiovascular system, eyes, nervous system, endocrine system, hematological system etc.
· History of epilepsy (except children febrile seizure/convulsion)
· Known history of high intraocular pressure or angle closure glaucoma
· Psychoactive substance abuse or dependences within 1 year prior enrollment.
· Depressive episode due to other mental disorders or physical diseases.
· Bipolar disorder, rapid cycling/circulation
· Female patient during their pregnant and lactation period or childbearing potential during study.
· History of severe drug hypersensitivity.
· Patients cannot administrate drug according to medical order.
· HAMD total score decreased more than 25% from screening to baseline
· Use of Electroconvulsive therapy within half year prior enrollment.
· Known lack of efficacy to escitalopram by treatment before.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Phase 4
COLLECTION AND COMPILATION OF DATA
Source of data:
Patient interview
Hamilton rating scale for depression
Montgomery-Åsberg Depression Rating Scale
}Clinical Global impressions scale.
Patient case notes
Treatment chart
Method of collection of data
The patients satisfying the inclusion criteria were assessed for the severity of the illness using, (1) HAM-D scale which assess the score of the 17 symptoms of the disease and (2) CGI scale which classifies the patients onto different groups on the basis of the severity of the disease, (3) MADRS was originally a subscale of the Comprehensive Psychopathological Rating Scale.
Hamilton Rating Scale for Depression
The Hamilton rating scale is designed to be used only on patients already diagnosed as suffering from depression. It is used for quantifying the results of an interview, and its value depends on the skill of the interviewer in eliciting the information.
The scale contains 21 items. Each item is measured on a five-point or three-point scale, and the scores are summed. If the score is higher patients has severe depression rate.
Depending on the version used, there are either 17 or 21 items for which an interviewer provides ratings. Besides the interview with the depressed patient, other information can be utilized in formulating ratings, such as information gathered from family, friends, and patient records. Hamilton stressed that the interview process be easygoing and informal and that there are no specific questions that must be asked.
OBSERVATION & RESULT:
PATIENT DEMOGRAPHIC CHARACTERISTICS
SEX DISTRIBUTION
Table. 1
|
SEX |
CITALOPRAM |
ESCITALOPRAM |
TOTAL NO.OF PATIENTS |
TOTAL PERCENTAGE |
|
MALE |
8 |
8 |
16 |
40% |
|
FEMALE |
12 |
12 |
24 |
60% |
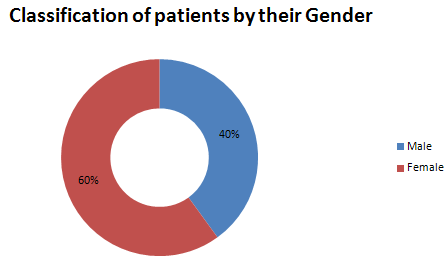
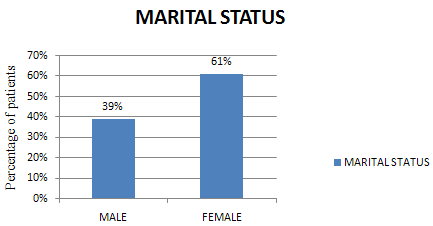
Out of the 40 major depressions Patients 16(40%) were males and 24(60%) were females. The numbers of female patients were higher when compared to male patients .this result shows us that female patient was mostly affected by depression. See in table.1
Figure. 1
AGE GROUP
Table. 2
|
Age group |
|
Severity of illness |
Total no. of patients |
Percentage |
||
|
Borderline mentally ill |
Mildly ill |
Moderately ill |
Markedly ill |
|||
|
20-30 |
2(20%) |
4(40%) |
2(20%) |
2(20%) |
10 |
25% |
|
31-40 |
3(25%) |
7(58.33%) |
0(0%) |
2(16.66%) |
12 |
30% |
|
41-50 |
2(15.38%) |
6(46.15%) |
3(23.07%) |
2(15.38%) |
13 |
32.5% |
|
51-60 |
1(25%) |
3(75%) |
0(0%) |
0(0%) |
4 |
10% |
|
61-70 |
0(0%) |
0(0%) |
1(100%) |
0(0%) |
1 |
2.5% |
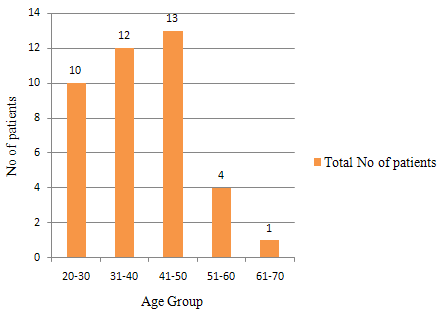
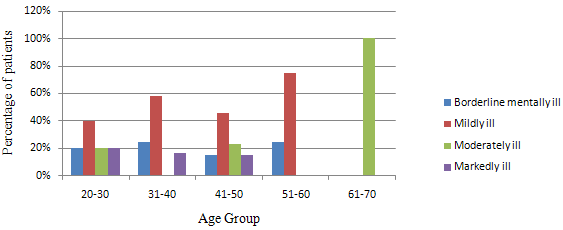
Out of the 40 patients 10(25%) patients were under the age of 20-30, 12(30%) patients were under the age group of 31-40, 13(32.5%)patients were under the age of 41-50, 4(10%) patients were under the age group of 51-60, and 1(2.5%) was under the age group of 61-70. Table.2 data’s shows that the maximum number of patients were under the age groupof 41-50.
Figure. 2
CLASSIFICATION OF PATIENTS BY THEIR AGE GROUP
Figure.3
MARITAL STATUS
Table. 3
|
MARITAL STATUS
|
NO. OF PATIENTS |
MALE |
FEMALE |
PERCENTAGE |
|
MARRIED |
36 |
14 |
22 |
90% |
|
UNMARRIED |
4 |
2 |
2 |
10% |
Of the 40 patients, 36(90%) were married and 4(10%) were Unmarried. This data’s clearly shows that most of married persons in this study were affected by depression, 14 males and 22 females were married so we came to know females were mostly affected by this disorder
Figure.4
OCCUPATIONAL STATUS
Table. 4
|
OCCUPATION |
NO. OF PATIENTS |
PERCENTAGE |
|
HOUSE WIFE |
20 |
50% |
|
BUSINESS |
8 |
20% |
|
PRIVATE EMPLOYEES |
4 |
10% |
|
GOVERNTMENT EMPLOYEES |
0 |
0% |
|
STUDENT |
0 |
0% |
|
AGRICULTURE |
3 |
7.5% |
|
UNEMPLOYED |
5 |
12.5% |
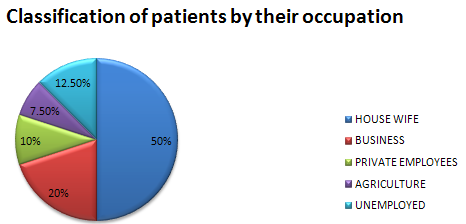
Of the 40 patients, 20(50%) were house wife, 8(20%)patients were business men, 4(10%) patients were private employees, 3(7.5%) patients were agriculturist and 5(12.5%) patients were unemployed. This data shows that the maximum numbers of patients were housewives because they were not had a chance to share their feelings to any else, they dump their feelings themselves; it was create a depressive mind.
Figure.5
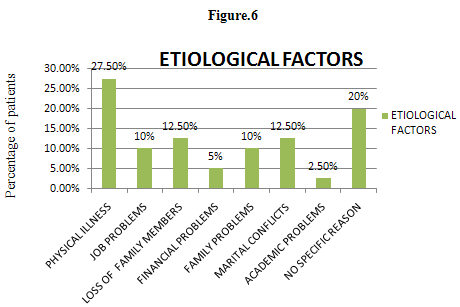
ETIOLOGICAL FACTORS
Table. 5
|
FACTORS |
NO. OF .PATIENTS |
PERCENTAGE |
|
PHYSICAL ILLNESS |
11 |
27.5% |
|
JOB PROBLEMS |
4 |
10% |
|
LOSS OF CLOSE FAMILY MEMBERS |
5 |
12.5% |
|
FINANCIAL PROBLEMS |
2 |
5% |
|
FAMILY PROBLEMS |
4 |
10% |
|
MARITAL CONFLICTS |
5 |
12.5% |
|
ACADEMIC PROBLEMS |
1 |
2.5 |
|
NO SPECIFIC REASON |
8 |
20 |
Out of the 40 patients, 11(27.5%) patients had physical illness as the etiological factor for depression.5(12.5%) patients had marital conflict, 4(10%) patients had problems associated with job, 5(12.5%) patients were had a problem of loss of a close family member, 2(5%) patients had financial problems, 4(10%) had family problems, 1(2.5%) had academic problems and 8(20%) patients had no specific reasons as the etiological factor in table.5
Figure.6
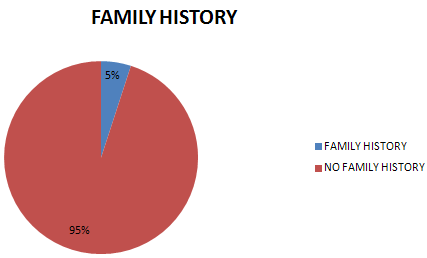
FAMILY HISTORY
Table. 6
|
CATEGORY |
NO.OF.PATIENTS |
PERCENTAGE |
|
FAMILY HISTORY |
2 |
5% |
|
NO FAMILY HISTORY |
38 |
95% |
Out of 40 patients 2(5%) patients had a close relative with depression whereas 38(95%) had no family history. This data shows clearly us depression was not a genetical disorder.
Figure.7
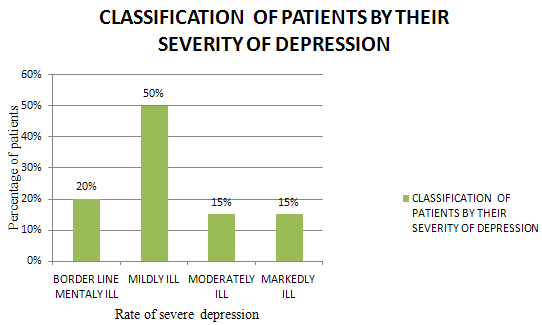
SEVERITY OF DISEASE
CLASSIFICATION OF PATIENTS ACORDING TO THE SEVERITY OF ILLNESS
Table. 7
|
SEVERITY OF ILLNESS |
NO.OF.PATIENTS |
PERCENTAGE |
|
BORDER LINE MENTALY ILL |
8 |
20% |
|
MILDLY ILL |
20 |
50% |
|
MODERATELY ILL |
6 |
15% |
|
MARKEDLY ILL |
6 |
15% |
On comparing the patients according to the severity of depression, more number of patients who came for treatment was mildly depressed (50%) followed by Border line mentally depressed (20%).The number ofModerately &Markedly depressed patients were (15%). The graphical representation in figure.9
Figure.8
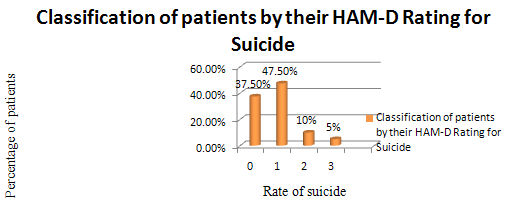
CLASSIFICATION OF PATIENTS ON THE BASIS OF HAM-D RATING FOR SUICIDAL TENDENCY
Table. 8
|
HAM-D RATING FOR SUICIDE |
ESCITALOPRAM |
CITALOPRAM |
TOTAL NO.OF.PATIENTS |
% |
|
0 |
10 |
5 |
15 |
37.5% |
|
1 |
7 |
12 |
19 |
47.5% |
|
2 |
1 |
3 |
4 |
10% |
|
3 |
0 |
2 |
2 |
5% |
Out of 40 patients who had a suicidal tendency, 15(37.5%) patients had HAM-D rating of 0(Absent) according to this 15 patients were not had any suicidal ideas. 19(47.5%) patients had HAM-D rating of 1(Feels that life is not worth living). 4(10%) patients had HAM-D rating of 2(Wishes he/she were dead or any thoughts of possible death to self). and 2(5%)patients had HAM-D rating of 3(Suicide ideas or gestures), according to before statement severe suicidal tendency was very less in both the drugs but comparatively citaloprm taking patients had suicide ideas or gestures.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to PharmaTutor Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Figure.9
DISTRIBUTION OF PATIENTS ACCORDING TO THE DRUG PATTERN
Table. 9
|
DRUG CATEGORY |
NAME OF THE DRUGS |
NO. OF. PATIENTS |
RESPONDER |
NON RESPONDER |
|
SELECTIVE SEROTONIN RE-UPTAKE INHIBITOR(SSRI) |
ESCITALOPRAM |
20 |
17(85%) |
3(15%) |
|
CITALOPRAM |
20 |
10(50%) |
10(50%) |
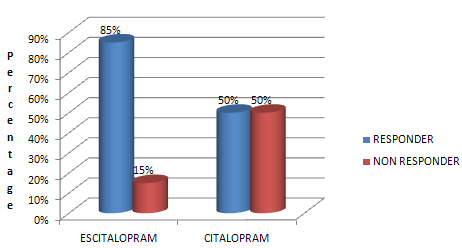
Out of 40 patients 20 patients were treated with Escitalopram in this 17 (85%) patients were responders, 3(15%) were non responders. Another 20 patients were treated with Citalopram in this 10(50%) patients were responders, 10(50%) were non responders. This result was shows us that Escitalopram taken patients had improved more in number compare to citalopram.
Figure.10
EFFICACY OF THE DRUGS CITALOPRAM 20MG AND ESCITALOPRAM 10MGBASELINE VALUES
|
DRUG |
HAMD |
MADRS |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
CITALOPRAM (Group A) |
27.75 |
2.2 |
32.4 |
3.46 |
|
ESCITALOPRAM (Group B) |
29.7 |
4.7 |
34.75 |
3.67 |
|
þ |
0.0227 Not Significant |
0.0220 Not Significant |
||
Table. 10
In this group A patients had a Mean value of 27.5 and SD value of 2.2 for HAMD scale. Mean value of 32.4 and SD value of 3.46 for MADRS scale. Group B patients had a Mean value of 29.9 and SD value of 4.7 for HAMD scale. Mean value of 34.75 and SD value of 3.67 for MADRS scale. Þvalue for both groups in HAMD scale is 0.0227 and MADRS scale is 0.0220. These results were shows us that both the drugs in baseline visit had no significant effects.
PERCENTAGE OF CHANGES IN HAMD DURNG SECOND VISIT
Table. 11
|
HAMD |
CITALOPRAM (Group A ) |
ESCITALOPRAM (Group B) |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
Baseline (First visit) |
27.75 |
2.2 |
29.7 |
4.7 |
|
Second visit |
25.15 |
3.3 |
23.7 |
8.39 |
|
Change |
2.6 |
3.1 |
6.2 |
8.8 |
|
% of change |
9.17 |
10.82 |
19.78 |
|