About Author: Main author: Amar Nagesh Kumar,
About Author: Main author: Amar Nagesh Kumar,
Lecturer, Department of Biochemistry,
SSR Medical College, Belle Rive, Mauritius
Co-author: Robby Kumar,
Lecturer, Department of Biochemistry,
SSR Medical College, Belle Rive, Mauritius
Abstract
Objective: To correlate serum magnesium levels among pregnant women with increasing parity and comparison of magnesium levels in rural and urban areas of Guntur district, Andhra Pradesh, India.
Materials and Methods: A total of 100 pregnant women with pregnancy duration of 24 weeks and more were enrolled for the study. Blood from the antecubital vein was drawn and serum magnesium levels were estimated by the colorimetric method.
Results: In all, 48% of the pregnant women had serum levels less than the normal level (1.80 mg/dl). There was a significant decrease in serum magnesium levels with the increase in parity. But no significant decrease of magnesium level in serum was found when compared among rural and urban pregnant women.
Conclusion: A high prevalence of magnesium deficiency was found among the pregnant women. But there was no significant change of serum magnesium levels when compared among pregnant women of rural and urban areas.
Reference ID: PHARMATUTOR-ART-1115
Introduction
Pregnancy is a physiological condition where serum magnesium levels are decreased. The decrease in magnesium level in blood is very significant during the third trimester because of hemodilution. The serum magnesium levels show no gestational age dependence until 30 weeks at which point it continuously declines. Generally the hypo magnesemia in most preganant women is associated with hemodilution , renal clearance during pregnancy and consumption of minerals by growing fetus [1, 2] . Magnesium has been established as an essential element for fetal well-being. Its deficiency during pregnancy has been reported to be associated with eclampsia, pre-eclampsia, preterm births, increased maternal hospitalization, incidence of low birth weight and small for gestational age infants[3, 4]. The administration of magnesium sulphate helps in the treatment of convulsions [5].Trials have documented that oral magnesium supplementation during pregnancy reduces hypertension miscarriage, prenatal birth and fetal growth retardation [3, 6]. Magnesium is considered as a rational agent for the prevention and treatmentof eclamptic seizures and also is drug of choice for prophylaxis [7].
The indication for magnesium therapy in the study by Lucas et al was a blood pressure of more than 140/90 mmHg, during labour. An approach based on this criteria would result in the treatment of many women with pre eclampsia who could not actually have seizures [8, 9]. Limited data is available on the serum levels of magnesium among pregnant women from the rural communities of, India. Hence, the present study was conducted.
Methods
Pregnant women from the rural areas and urban places were selected for the study. Basic information like Age, Weight, Parity, Risk factors, life style etc., was taken from the individuals by approved signed consent forms.
The cross sectional study was conducted in the section of Obstetrics and Gynecology at katuri Medical College & Hospital, Guntur. The present study was carried out in hundred pregnant women admitted in OBG ward and at the out patient department at KMC&Hospital, Guntur. The studied population consists of 25 women with out pregnancy. They are taken as controls. 40 are belongs to first parity, another 40 are 2nd parity and 20 are of 3rd parity. Informed consent from the pregnant women was taken to participate after explaining the objective of the study.
About 3ml blood was collected from the antecubital vein from the subjects with disposable syringes into a clean, dry glass vial or in a centrifuge tube. The blood samples were centrifuged immediately at 3500rpm for 10min to separate serum. The serum is stored at 40Cin refrigerator until analysis.
Serum magnesium levels were estimated by utilizing the colorimetric method of A.j Smith 1955 using Eryochrome block T dye. The results of control and standards are plotted and unknowns are read from the graph.The data collected was subjected to statistical tests of mean and standard deviation were done using SPSS Software 17.0 and Pearson correlation was used for correlating different parameters. Serum samples with magnesium levels less than 1.8mg/dl were considered as deficient of magnesium nutriture[10].
RESULTS
A total of 100 pregnant women with pregnancy duration of 24 weeks and more were enrolled for the study. The mean age of the pregnant woman was 23.2±3.3 years. Of these 53% was pregnancy duration less than 32 weeks. Almost 60% of women had parity 2 or more. About 25 women without pregnancy were considered as controls. Their mean serum magnesium levels are 2.49 ±0.29 mg/dl. The mean serum magnesium level of pregnant women was 1.89±0.42 mg/dl. Serum samples with magnesium levels less than 1.8 mg/dl were considered as deficient of magnesium nutriture[11, 12]. About 48% (n=100)of the pregnant women had serum magnesium levels less than 1.8mg/dl. There was a significant decrease (p<0.0001) in serum magnesium with the increase in parity.Primiparous pregnant women, mean serum magnesium values are 1.77±0.34mg/dl. Serum magnesium levels of pregnant women with 2nd and 3rd parity were 1.58±0.19, 1.52±0.26 mg/dl respectively(Table 1). Pregnant women with parity 2 and more had a significantly lower serum magnesium level, when compared to controls.
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE
Based on the urban and rural areas, a comparative study was also made on their socio economic status. Of the 100 pregnant women, 65% are belongs to low socio economic status from rural area and remaining 35% are belongs to high economic status from urban area. The mean serum magnesium levels in low socioeconomic status are 1.63±0.31. Whereas the mean serum magnesium values in high socio economic status is 1.75±0.41. The serum magnesium levels had shown slight decrease in both rural and urban pregnant women cases compared to controls but not significant statistically (p ?0.05) (Table 2).
DISCUSSION:
Present study, shows that there is a decrease in serum magnesium with the increase in parity. previous study reported that frequent cycles of reproduction exert a significant stress leading to a greater risk of undernutrition among the pregnant women[13]. Earlier studies have also reported similar findings[12, 14]. Correlation study (table) has revealed significant positive correlation of serum magnesium level with increasing parity. The haemodilution during the last trimester of pregnancy could be another contributing factor leading to a higher prevalence of deficiency of magnesium[12, 14]. Thus this study concludes that the serum magnesium levels decreases with the increase in parity and does not make any difference with the socio economic status. Statistically it has proven that the decrease was not significant, but clinically we suggest it is was a decrease, as the patients were having complications like eclampsia, pre-eclampsia.
References
1. Givens MH, Macy IG: The chemical composition of the human fetus. J Biol Chem 102,7-17, 1933.
2. Coons CM, Coons RR: Some effects of cod liver oil and wheat germ on the retention of iron, nitrogen, phosphorus, calcium and magnesium during human pregnancy. J Nutr 10,289-310, 1935.
3. Almonte RA, Heath DL, Whitehall J, Russell MJ, Patole S & Vink R: Gestational magnesium deficiency is deleterious to fetal outcome. Biol. Neonate 76, 26–32, 1999.
4. Makrides M & Crowther CA: Magnesium supplementation in pregnancy, 2000.
5. The Magpie Trial Collaboration Group: Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet. 359, 1877–1890, 2002.
6. Wynn A & Wynn M: Magnesium and other nutrient deficiencies as possible causes of hypertension and low birth weight. Nutr. Health 6, 69–88, 1988.
7. Prithard JAthe use of magnesium ion in the management of eclmptogenic toxemias.Gynecol.Obstet, 40,100-131, 1995
8. Lucas.M.J, Levenok.J,cuunigham F.G a comparision of magnesium sulfate with phenytoin for the prevention of eclampsia .N.Engla J Med 333,201-205,1995.
9. Ladefoged K, Hessov I, Jarnum S. Nutrition in short-bowel syndrome. Scand J Gastroenterol Suppl, 216:122-31,1996.
10. A J .Smith, A colorimetric method for the estimation of serum magnesium. Biochem J, 60(3):522 – 527,1955.
11. Elmer P & Conn N: Analytical Methods for Atomic Absorption Spectrophotometry, pp 273–290, 1975. London: Oxford Press.
12. P Pathak, S K Kapoor, U Kapil and S N Dwivedi Serum magnesium level among pregnant women in a rural community of Haryana State, India. European Journal of Clinical Nutrition 57, 1504–1506, 2003.
13. Merchant K & Martorell R: Frequent reproductive cycling: does it lead to nutritional depletion of mothers? Prog. Food Sci. Nutr. Sci. 12, 339–369, 1988.
14. Chesley LC: Plasma and red blood cell volumes during pregnancy. Am. J. Obstet. Gynecol. 112, 440–450, 1972.
Table: 1 serum magnesium level with increase in parity
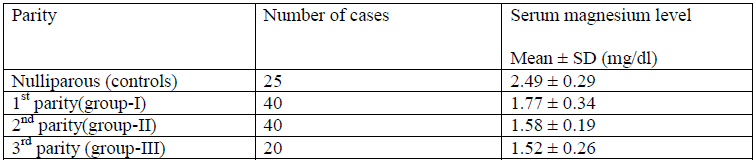
Table:2 comparison of serum magnesium levels among rural and urban pregnant women

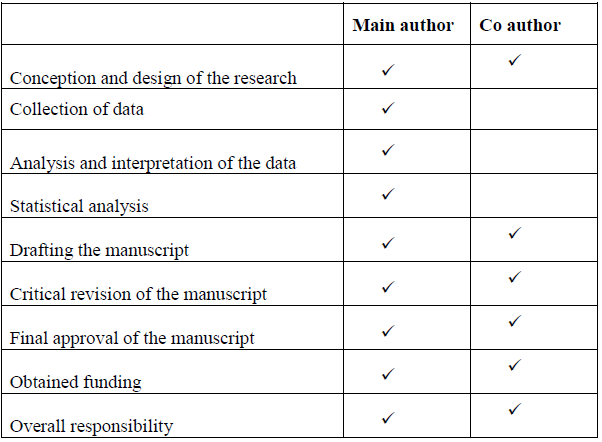
Authors' Contribution Statement
NOW YOU CAN ALSO PUBLISH YOUR ARTICLE ONLINE.
SUBMIT YOUR ARTICLE/PROJECT AT articles@pharmatutor.org
Subscribe to Pharmatutor Job Alerts by Email
FIND OUT MORE ARTICLES AT OUR DATABASE