About Authors
Avdesh Thassu
MPharm (Nat. Chem.); MBA(Mkt.)
Associate Vice President
Global Regulatory Affairs,
Emami Limited,
7044455199
athassu@hotmail.com
Chandra Mohan Nandi
MSc. (Organic Chem.)
Deputy Manager,
Global Regulatory Affairs,
Emami Limited,
9051706947
chandramohannandi@yahoo.in
Abstract :
Hair fall is a very common disorder nowadays. It can be caused by a variety of reasons that can be congenital or acquired.It is a common cosmetically and psychosocially distressing condition, however, there are limited studies on its prevalence in the Indian subcontinent. The main aim of this article is to determine the factors associated with hair fall &highlightinghair rejuvenation strategies,and hair growth management too.
Introduction
Almost every people in the world wants luxurious hair with youth and beauty. But due to some internal & external factors, all the males & females is not getting their desired hair & they are facing hair loss problem. Male pattern hair loss or Androgenic Alopecia (AGA), is the most common type of hair loss in men andFemale pattern hair loss (FPHL) is the most common form of alopecia in women.
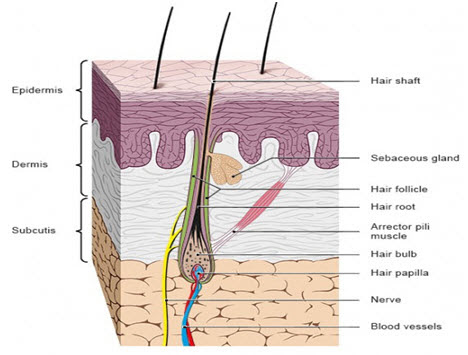 Hair Structure : Each hair has a shaft and a root. The shaft is the observable part of hair that sticks out of the skin. The hair root is deepens into the skin and extends down to inner layers of the skin. It is surrounded by the hair follicle, which is also connected to a sebaceous gland. Each hair follicle is involvedin a minute muscle, called arrector pili, which can make the hair arise. The nerves present in that part, can sense hair movement even sensitive to the slightest draft. At the base, the hair root widens to forma round hair bulb. Hair papilla supplies blood to the hair root, is found inside the bottom of the hair bulb.
Hair Structure : Each hair has a shaft and a root. The shaft is the observable part of hair that sticks out of the skin. The hair root is deepens into the skin and extends down to inner layers of the skin. It is surrounded by the hair follicle, which is also connected to a sebaceous gland. Each hair follicle is involvedin a minute muscle, called arrector pili, which can make the hair arise. The nerves present in that part, can sense hair movement even sensitive to the slightest draft. At the base, the hair root widens to forma round hair bulb. Hair papilla supplies blood to the hair root, is found inside the bottom of the hair bulb.
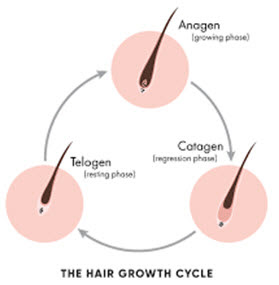 Hair Growth Cycle : As far as new hair cells continue to grow in hair bulb, the hair continues to grow longer. This development phase is called the anagen phase. At any point of time, about 90% of a person’s total amount of hair is in this phase.
Hair Growth Cycle : As far as new hair cells continue to grow in hair bulb, the hair continues to grow longer. This development phase is called the anagen phase. At any point of time, about 90% of a person’s total amount of hair is in this phase.
At the end of the growth phase, the hair root is isolated from the papilla. Then a transitional phase calledcatagen phase starts, lasting about two to four weeks. The supply of blood is cut off in the final resting phase, calledtelogen phase. In this phase, the hair is gradually pushed out of the skin and ultimately falls out.
What causes increased hair loss : The rate of hair fall may increase prominently if the hair roots are damaged during the growth phase or if a lot of hairs go into the resting phase at the same time. If no replacementof the hairis done, that part of the skin becomes bald. This kind of hair loss is calledalopecia.
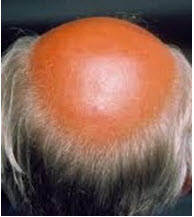
 Male Pattern Baldness : The genetic condition is the most common of all hair loss conditions, commonly known by the medical term as androgenic alopecia(AGA), or more well-known phrase, male pattern baldness (MPB). The MPB gene and hair loss pattern are passed through the family from both the male and female sides. Primarily, it slows down the hair growth and then it reduced the hair quality and strength. Over time these two factors result in hair loss. The Norwood scale help depicts the various states of hair loss pattern of male.
Male Pattern Baldness : The genetic condition is the most common of all hair loss conditions, commonly known by the medical term as androgenic alopecia(AGA), or more well-known phrase, male pattern baldness (MPB). The MPB gene and hair loss pattern are passed through the family from both the male and female sides. Primarily, it slows down the hair growth and then it reduced the hair quality and strength. Over time these two factors result in hair loss. The Norwood scale help depicts the various states of hair loss pattern of male.
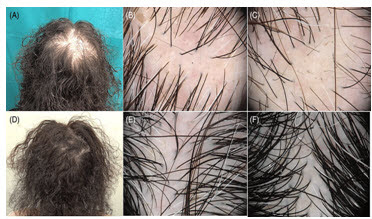
 Female pattern Baldness : A genetic hair loss condition for female known as androgenic alopecia or female pattern baldness. (FPB). The hair loss isactivated by the male hormone but is more complex compared to the male hair loss. It can occur anytime after puberty but is often seen after menopause.Women have approximately half the amount of 5-alpha reductase compared to men and this is thought to be one of the indicators of the difference in hair loss patterns between men and women. To help categorize the different stages of female pattern hair loss the Ludwig scalewas introduced. The scale indicates from mild thinning stage to more diffused patterns over the scalp
Female pattern Baldness : A genetic hair loss condition for female known as androgenic alopecia or female pattern baldness. (FPB). The hair loss isactivated by the male hormone but is more complex compared to the male hair loss. It can occur anytime after puberty but is often seen after menopause.Women have approximately half the amount of 5-alpha reductase compared to men and this is thought to be one of the indicators of the difference in hair loss patterns between men and women. To help categorize the different stages of female pattern hair loss the Ludwig scalewas introduced. The scale indicates from mild thinning stage to more diffused patterns over the scalp
Factors leading to hair loss :
Table-1 :
|
Factors |
Description |
|
Major physical–emotional stress |
Surgery, severe illness, diet or nutrition changes, and emotional stress can cause hair loss |
|
Chemotherapy |
Cholesterol-lowering drugs, Parkinson medications, anti-ulcer drugs, anticoagulants, agents for gout, anti-arthritic drugs derived from vitamin A, anticonvulsants for epilepsy, antidepressants, beta-blocker drugs, male steroids. |
|
Genetic predisposition |
A genetic component to androgenetic hair loss exists |
|
Dihydrotestosterone (DHT) |
Increased level of DHT (Dihydrotestosterone) shortens the hair cycle and progressively miniaturizes scalp follicles and this may be due to the atherosclerotic process blocking the microvasculature that nourishes the hair follicles |
|
Excessive sebum |
Excessive sebum causes a high level of 5-alpha reductase and pore clogging, thus malnutrition of the hair root |
|
Cardiovascular diseases |
High levels of LDL in cardiac patients are converted to 5-alpha reductase enzyme, which produces DHT from testosterone, causing hair loss |
|
Smoking |
Tobacco smoke damages the lining of blood vessels, leading to less production of nitric oxide and thus inducing hair loss |
Common acquired causes of hair loss :
 1. Telogen effluvium:It is one of the common causes of hair loss. This condition is characterized by diffuse hair shedding due to a disruption in the hair cycle. The daily hair loss can be up to 1000 hairs. Telogen effluvium can be due to iron deficiency, hypoalbuminemia, thyroid dysfunction. Usually, this condition affects females and children.
1. Telogen effluvium:It is one of the common causes of hair loss. This condition is characterized by diffuse hair shedding due to a disruption in the hair cycle. The daily hair loss can be up to 1000 hairs. Telogen effluvium can be due to iron deficiency, hypoalbuminemia, thyroid dysfunction. Usually, this condition affects females and children.
 2. Androgenetic alopecia:This is known as common balding. This condition is characterized by shedding and thinning of certain areas on scalp. This can affect both genders. It is due to progressive miniaturization of hair which means anadvanced transformation of the terminal (coarse) hair into vellus (fine) hair follicle. Male hormones (androgens) play an important role in inducing this condition in both sexes.
2. Androgenetic alopecia:This is known as common balding. This condition is characterized by shedding and thinning of certain areas on scalp. This can affect both genders. It is due to progressive miniaturization of hair which means anadvanced transformation of the terminal (coarse) hair into vellus (fine) hair follicle. Male hormones (androgens) play an important role in inducing this condition in both sexes.
 3. Alopecia areata:The main types of alopecia areata include localized bald area in the scalp, brows, or beard areas, baldness of the total scalp area and total body. A defect in the immune system, causing inflammation of the hair roots may be the causative factor for hair loss. Psychological and emotional changes may play a role in this condition.
3. Alopecia areata:The main types of alopecia areata include localized bald area in the scalp, brows, or beard areas, baldness of the total scalp area and total body. A defect in the immune system, causing inflammation of the hair roots may be the causative factor for hair loss. Psychological and emotional changes may play a role in this condition.
 4. Trichotillomania:It is a psychiatric disorder with a melancholic impulse to pull one’s own hair. There is a female prevalence with ratio of 3.5:1comapre to males & children.This condition can be considered as impulse-control disorder. If trichotillomania is detected, then the patient should be referred to consult a psychiatrist for further treatment.
4. Trichotillomania:It is a psychiatric disorder with a melancholic impulse to pull one’s own hair. There is a female prevalence with ratio of 3.5:1comapre to males & children.This condition can be considered as impulse-control disorder. If trichotillomania is detected, then the patient should be referred to consult a psychiatrist for further treatment.
 5. Tinea capitis:The word “Tinea” means fungal infection &capitis indicates the scalp. It is so called, since the lesions are arranged in rings. It is a common cause of hair loss in children. Tinea capitis is commonly caused by dermatophytes. Dermatophytes, invading the hair, are classified as favus, endothrix, or ectothrix. Favuscaused by Trichophytonschoenleinii, is an inflammatory condition, characterized by yellowish-crusted hairy plaques. Endothrix caused predominantly by Trichophytontonsurans, Trichophytonsoudanense, and Trichophytonviolaceumisseen when the fungus grows completely within the hair shaft.
5. Tinea capitis:The word “Tinea” means fungal infection &capitis indicates the scalp. It is so called, since the lesions are arranged in rings. It is a common cause of hair loss in children. Tinea capitis is commonly caused by dermatophytes. Dermatophytes, invading the hair, are classified as favus, endothrix, or ectothrix. Favuscaused by Trichophytonschoenleinii, is an inflammatory condition, characterized by yellowish-crusted hairy plaques. Endothrix caused predominantly by Trichophytontonsurans, Trichophytonsoudanense, and Trichophytonviolaceumisseen when the fungus grows completely within the hair shaft.
Strategies for hair growth and rejuvenation :
There are various drugs that may stimulate hair growth. It may increase the lineargrowth rate of hair, may increase the diameter of the hair fibre and alter the hair cycle. In surgical treatment methods, the introduction of micrografts and minigrafts has made a most significant advancement in the care of male pattern baldness and female androgenic alopecia. Additionally, many other applications in the reconstruction of facial and scalp hair have been found.
Role of nutrients and minerals in the prevention of hair loss :
Table-2
|
Nutrients and minerals |
Mechanism of preventing hair loss |
|
Niacin (vitamin B3) |
|
|
Vitamin B complex |
|
|
Ascorbic acid (vitamin C) |
|
|
Tocopherol (vitamin E) |
|
|
Zinc |
|
|
Essential fatty acids (primrose and salmon oil) |
|
|
Amino acids (L-cysteine and L-methionine) |
|
Synthetic drugs which helpwith hair growth :
Minoxidil : Minoxidil was first used in tablet form as a medicine to treat high blood pressure, but it was noticed that some patients being treated with minoxidil experienced excessive hair growth (hypertrichosis) as a side effect. Topical minoxidil (2,4-diamino6-piperidino pyrimidine-3-oxide) is the only drug approved by the Food and Drug Administration to treat male and female pattern baldness. The topicalsolution must be applied to the balding area twice a day, every day. Decreasing the dosage to once a day results in some hair loss, and discontinuing application causes regression to pre-treatment baldness within 3–6 weeks. The disadvantages of minoxidil are: (i) lifetime commitment; (ii) high cost: it is not covered by health insurance schemes as it is considered a cosmetic; (iii) its side effects – including itching and prickling, headaches, dizzy spells and, in some, heartbeat irregularities.
Pyridine derivatives:These include pinacidil, and nicorandil. They play a role in the hair growth cycle management.
Benzothiazide derivative:Oral diazoxide causes hypertrichosis in most hypoglycemic children and about 1% of adults, and induces some scalp hairs in 25% of the balding patients.
Steroids : Finasteride is a 4-aza steroidal drug which acts by inhibiting the 5-alpha reductase (enzyme) that transforms testosterone into the dihydrotestosterone (DHT) form, responsible for hair loss. Blocking the action of DHT seems to stimulate growth of stronger, thicker and more pigmented hair.They are type I 5-alpha reductase (located in the sebaceous glands) inhibitors but are not time-dependent like finasteride, which is a time-dependent inhibitor of type II 5-alpha reductase.
Side effects : When using any synthetic drugs, there possibly have some contraindications. Need to be concerned about that.Side effects of topical hair loss treatments like minoxidil can include: darkening of body hair, growth of body hair, irritation and dermatitis on the scalp, and effects on sexual health like low sex drive.
Natural products:Ancient ayurvedic ingredientshave been reported and documented as potent hair growth promoters. The natural products are reported to be more effective alternatives for hair growth therapy than the synthetic drugs.. Various natural products associated with hair growth activity are listed in Table 3.
Table 3
|
Herbal ingredient |
Hair growth activity |
|
Grape seed |
|
|
Rosemary oil |
|
|
Sage (Salvia officinalis) |
|
|
Aloe vera |
|
|
Green tea |
|
|
Saw palmetto (Serenoa repens) |
|
|
Hibiscus rosasinensis |
|
Conclusion : Diagnosis of hair fall and common baldness is not difficult. Background analysis and scalp examination are crucial for initial diagnosis and management. A child with a history of seborrheic dermatitis-like hair loss may have tinea capitis. The status of treatment of alopecia is the result of recent advances in our understanding of its aetiology and progression. Angiogenesis, androgen antagonism,vasodilation through potassium channel opening and 5-alpha reductase inhibition are the major non-surgical therapeutic strategies for hair growth promotion.Based on the technical evaluation, this article will help to understand the effect of natural ingredients to prevent the hair fall and improve hair growth management.
References :
• Lippert H. Lehrbuch Anatomie. Munich: Urban und Fischer; 2017.
• Menche N (Ed). BiologieAnatomiePhysiologie. Munich: Urban und Fischer; 2016.
• Pschyrembel. KlinischesWörterbuch. Berlin: De Gruyter; 2017.
• Dawber R (1995). Hair and scalp disorders, common presenting signs, differential diagnosis and treatment. 1st edition, Martin Dunitz. London, pp.11-16.
• Shapiro J (2002). Hair loss: principles of diagnosis and management of alopecia. 1st edition. Martin Dunitz Ltd, London, pp.1-18.
• Sperling LC (1991). Hair anatomy for the clinician. J Am AcadDerm, 25:1-17
• Hair growth and rejuvenation: An overview Article in Journal of Dermatological Treatment • June 2011 DOI: 10.3109/09546630903578574 • Source: PubMed
• Rushton H, Ramsay H (1992). The importance of adequate serum ferritin levels during oral cyproterone acetate and ethinylestradiol treatment of diffuse androgen-dependent alopecia in women. ClinEndocrinol, 26:421-427.
• Dawber R (1995). Hair and scalp disorders, Common presenting signs, differential diagnosis and treatment. 1st edition, Martin Dunitz. London, pp.96-106.
• Whiting DA (1998). Male pattern hair loss: current understanding. Int J Derm, 37:561-566.
• Olsen E (2001). Female pattern hair loss. J Am AcadDerm, 45 (3, Suppl 1):70-80.
• Sperling L (1996). Evaluation of hair loss. CurrProbDerm, 8(3): 97-136.
• Shapiro J, Price VH (1998). Hair regrowth, therapeutic agents. DermatolClin, 16 (2): 341-356.
• Shapiro J (2002). Hair loss: principles of diagnosis and management of alopecia. 1st edition, Martin Dunitz. London, pp. 102-104.
• Roberst JL (1997). Androgentic alopecia in men and women: an overview of causes and treatment. Dermatology nursing, 9(6): 379-378
• Callan AW, Montalto J (1995). Female androgenetic alopecia: an update. Aust J Dermatol, 36 (2):51-55
• Muller SA (1990). Trichotillomania: a histopathologic study in sixty-six patients. J Am AcadDermatol, 23:56-62.
• Elewski BE (2000). Tinea capitis: A current perspective. J Am AcadDerm, 42 (1 Pt 1):1-18
• Ocampo-Garza SS, Vastarella M, Nappa P, Cantelli M, Fabbrocini G. Telogen effluvium in the new SARS-CoV-2 era. Int J Dermatol. 2021; 60:e265-e266. https://doi.org/10.1111/ijd.15482
• Hair growth and rejuvenation: An overview Article in Journal of Dermatological Treatment • June 2011 DOI: 10.3109/09546630903578574 Source: PubMed